Article Text

Statistics from Altmetric.com
Editor—Silver-Russell syndrome (SRS) is characterised by severe intrauterine growth retardation (IUGR), postnatal short stature, asymmetry of the face, body, and limbs, short and incurved fifth fingers, and a characteristic triangular face with a prominent and bossed forehead, a small lower jaw, and downturned corners of the mouth.1 2 Many other slightly dysmorphic features are seen in SRS patients (table 1) and these have been regarded mostly as confirmatory, not obligatory, for the diagnosis.3-5 Any one feature is not consistently observed in all SRS patients and the expression of features tends to vary greatly among subjects leading to considerable heterogeneity.3 4 Straightforward criteria for the evaluation of the severity of SRS characteristics have not been set and it has been proposed that SRS might in fact comprise different subgroups.4 6 Most SRS cases are sporadic, but different monogenic modes of inheritance have been proposed.7-9Abnormalities of chromosomes 8, 15, 17, and 18 have also been associated with SRS.10-15
Occurrence of SRS features. Categorisation is based on multiple published reports of SRS features, on the general emphasis stated in these reports for inclusion criteria in SRS studies, and on our own observations
Maternal uniparental disomy of chromosome 7 (matUPD(7)), the inheritance of both copies of chromosome 7 exclusively from the mother, occurs in approximately 10% of Silver-Russell syndrome (SRS) patients.16-19 Altogether, 21 cases of matUPD(7) have been reported6 16-24 and at least 14 of these have been diagnosed with SRS.6 16-19 All matUPD(7) patients have pre- and postnatal growth retardation, except one case who had short stature only postnatally.23 Paternal uniparental disomy of chromosome 7 has no effect on growth and development.25 It has been suggested that there is at least one imprinted gene influencing growth and development on chromosome 7. MatUPD(7) patients presumably end up with two copies of the maternally imprinted gene and thus lack the effects of a growth promoting gene. To date, three imprinted genes, PEG1/MEST,γ2-COP, andGRB10, are known on chromosome 7, but their role in SRS remains undecided.26-29
In a systematic screening for cases of matUPD(7) among patients with SRS, we have identified four matUPD(7) cases out of 32 SRS patients studied, consistent with a frequency of approximately 10%. These four matUPD(7) patients present with many common characteristics and seem to form a phenotypically homogeneous group. They consistently lack some classical features of SRS, such as a significantly triangular face, micrognathia, and downturned mouth corners. However, all present with additional specific features such as speech delay, severe feeding difficulties, and excessive sweating. We sought to evaluate which typical SRS features are most predominant in matUPD(7) patients and if these features differentiate a matUPD(7) phenotype from non-matUPD(7) SRS patients.
Patients were recruited from the outpatient clinic for growth disorders at the Hospital for Children and Adolescents, University of Helsinki, Finland. The diagnosis of SRS was confirmed in all patients either by a paediatric endocrinologist or by a medical geneticist. Patients were included in this study using the following criteria: (1) intrauterine growth retardation and/or born small for gestational age, (2) postnatal growth retardation exceeding −2.5 SD, and (3) at least three of the following facial characteristics: triangular face, micrognathia, frontal bossing, craniofacial disproportion in early infancy, and relative macrocephaly, and (4) at least one of the following relative criteria: asymmetry, hemihypertrophy, clinodactyly/brachydactyly of the fifth digits, low set ears, and hypospadias/cryptorchidism. All patients were also required to have normal karyotype, growth hormone excretion, and thyroid function. Patients and their parents provided written informed consent and blood samples were obtained from the patients and parents. The study was approved by the ethical review board of the Hospital for Children and Adolescents, University of Helsinki, Finland.
We genotyped all SRS patients on blood DNA with 14 chromosome 7 specific fluorescent tetra- and dinucleotide repeat microsatellite markers by PCR and an automated sequencer (ABI). Maternal only inheritance of chromosome 7 was detected in four SRS patients out of 32 studied (12.5%). Complete isodisomy was observed in case I and mixed hetero- and isodisomy in the other three cases (fig 1). Correct paternity was verified for all matUPD(7) patients by genotyping 12 chromosome 18 microsatellite markers in a similar way.
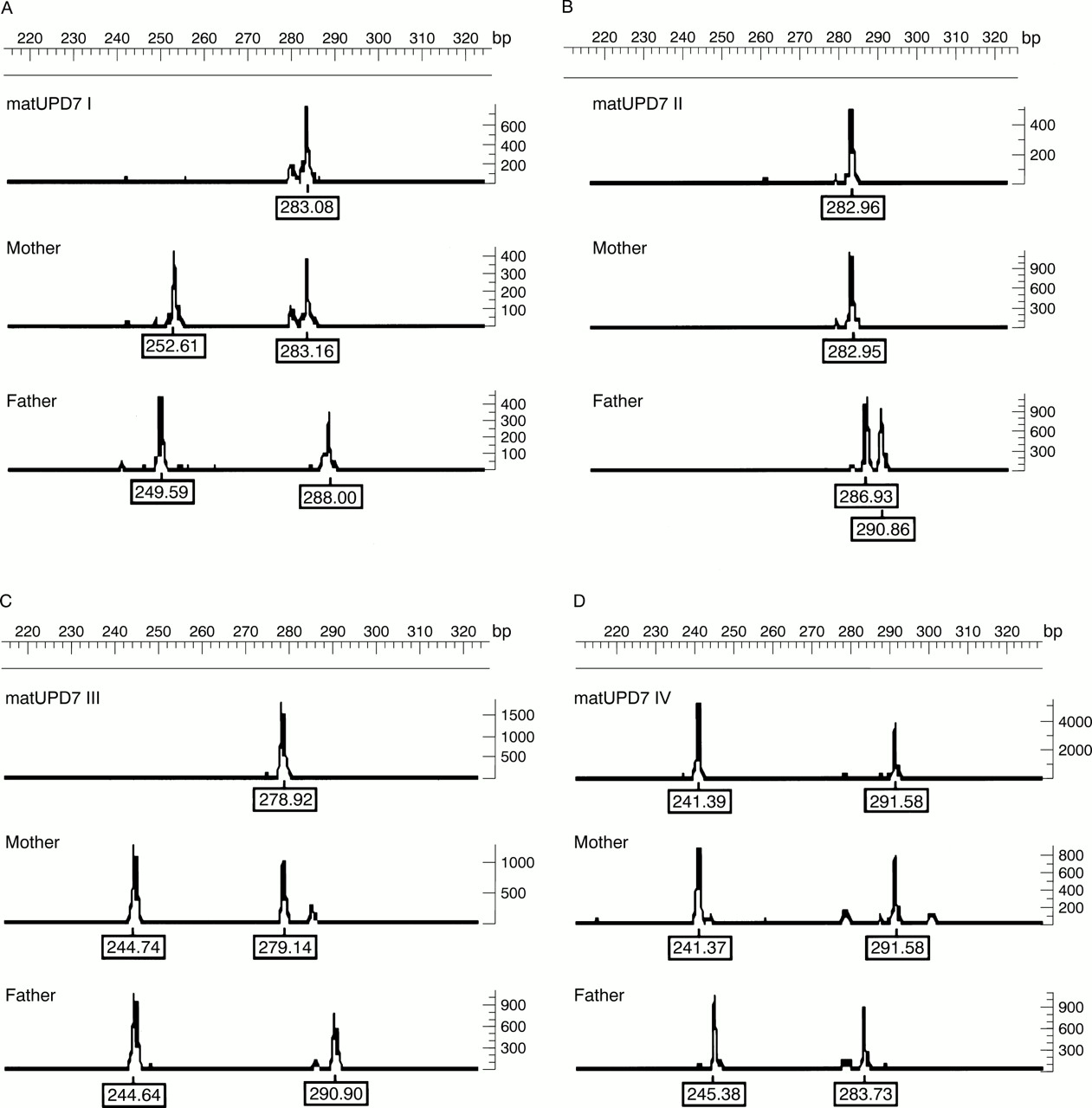
Microsatellite marker D7S2195 (7q35) indicating matUPD(7). Microsatellite markers spanning chromosome 7 showed complete maternal isodisomy in matUPD(7) I and mixed iso- and heterodisomy in matUPD(7) II, III, and IV. (A, C) the probands are homozygous for the larger maternal alleles and have inherited two copies of one maternal chromosome 7 (isodisomy). (B) The proband and the mother are both homozygous for the same allele. Isodisomy and heterodisomy are both possible and it is impossible to discern if the proband has inherited two copies of one maternal chromosome 7 (isodisomy) or both maternal chromosomes (heterodisomy). (D) The proband is heterozygous and shares both alleles with her mother and therefore has inherited both maternal chromosomes 7 (heterodisomy). Marker D7S2195 was fluorescently labelled and analysed by automated detection systems (ABI and Genotyper).
We evaluated the patients by reviewing medical data and growth charts. Nine patients were further evaluated by structured interviews and physical examinations. At the last evaluation, the matUPD(7) patients I, II, III, and IV were 19.0, 3.0, 2.8, and 4.4 years old, respectively (average 7.3 years), and the average age of non-matUPD(7) SRS patients was 9.9 years (range 0.8-19.0 years). The clinical parameters evaluated are listed in table 2. Dental age and craniofacial structures of matUPD(7) patients I-III were examined clinically and from photographs, lateral cephalograms, and orthopantomograms by an experienced orthodontist (SP) in comparison to a cohort of 19 SRS patients.30 All the SRS patients were sporadic cases and their sibs had normal growth and development. No significantly short relatives were known in any of the families. Maternal and paternal ages at the time of birth were exceptionally high in matUPD(7) cases (average maternal age 41 years and average paternal age 44 years) compared to non-matUPD(7) SRS patients (average maternal age 29 years and average paternal age 31 years).
Percentage of typical SRS features observed in our matUPD(7) patients and non-matUPD(7) SRS cases, previously reported matUPD(7) cases,16-24 and generally in SRS (three reports). Only findings that were clearly mentioned in each report have been included in these figures. Features not clearly mentioned in patient records or in reports of SRS patients were regarded as not present. However, it is uncertain whether these characteristics were truly missing or if they had not been evaluated. For one SRS patient with matUPD(7) no clinical findings were reported,17 so the numbers of previously reported matUPD(7) patients in this table is 20
All matUPD(7) patients were born SGA and had significant postnatal growth retardation (average −4.3 SD at 2 years of age) (table 3). The matUPD(7) patients were diagnosed with SRS in early childhood based on typical SRS features: a broad and high forehead, low set and posteriorly rotated ears, relative macrocephaly, craniofacial disproportion (observed both visually as a small face in relation to the head and also radiologically by a discrepancy of skull size to facial bone structure) in early infancy, and the left leg is shorter (0.5-1 cm) than the right. They all suffered from severe feeding difficulties and excessive sweating. All had speech delay particularly with problems in articulation.
Auxological data of matUPD(7) and non-matUPD(7) SRS patients
Patient I (fig 2A, B, M) was born at 36 weeks' gestation. He had slight motor and neuropsychological developmental delay and speech delay with marked problems in articulation. At the age of 13.5, WISC-R showed an IQ of 94 with a discrepancy between verbal (IQ 88) and non-verbal skills (IQ 102). Additional neuropsychological evaluation showed dysphasia-like problems caused by difficulties in articulation, mostly because of dyspraxia in the vocal muscles, and significant problems in finding the appropriate words. Dyspraxia in hand movements and clumsiness in motor skills was also noted. At the age of 19 he has trouble finding the correct words and his speech is slightly incoherent. He has concluded a primary education and is currently enrolled in an adjusted school in health care. He had bilateral undescended testes, which were successfully treated.X rays showed slender long bones, a hypoplastic sacrum, an absent coccyx, and only four lumbar vertebrae. He has clino- and brachydactyly of the fifth digits, a short neck, short upper arms, slight facial asymmetry with left side hypertrophy, and slight right sided trunk and limb hemihypertrophy. At 10.9 years he had a delayed dental age of 9.1 years (−2.2 SD). He received growth hormone (GH) therapy from the ages of 8.6 to 12.8.

{kind=link}
{kind=link}
MatUPD(7) patients (A-H) share a similar facial appearance and lack the classical SRS features of micrognathia, downturned mouth corners, and a triangular face seen in non-matUPD(7) SRS patients (I-L). All matUPD(7) patients have low set and posteriorly rotated ears (B, D, F, H). MatUPD(7) patients (M, N) have a sturdy appearance and lack the leanness typical of SRS which is observed in non-matUPD(7) patients (O, P). (A, B) MatUPD(7) I aged 5.5 years, (C, D) matUPD(7) II aged 2.3 years, (E, F) matUPD(7) III aged 1.7 years, (G, H) matUPD(7) IV aged 4.4 years, (I, J) SRS case 1 aged 1.4 years, (K, L) SRS case 2 aged 6.2 years, (M) matUPD(7) I aged 5.5 years, (N) matUPD(7) III aged 1.7 years, (O) SRS case 1 aged 1.4 years, (P) SRS case 2 aged 6.2 years. Written consent for publishing the photographs was received from all families.
Patient II (fig 2C, D) was born at 35+3 weeks' gestation. His psychomotor development is normal but he has speech delay, with mainly multiple articulation problems. He has brachy- and clinodactyly of the fifth digits, a short neck, short upper arms, and slight right side facial and limb hemihypertrophy. His first tooth erupted at the age of one year (−1.5 SD) and at 4.2 years his dental age was 3.6 (−0.8 SD). Slender long bones, round and short hand bones, and exceptionally short fifth metacarpals and phalanges were seen onx ray.
Patient III (fig 2E, F, N) was born at 39+3 weeks' gestation and her neonatal period was marked by excessive vomiting and regurgitation. She had gross feeding difficulties up to the age of 4.5 months, mainly because of deficient sucking, and feeding times reached up to 1.5 hours. Her psychomotor development is otherwise normal but she has marked speech delay, mainly in producing speech. She understands speech well, but produces only rare one or two word sentences, and communicates mostly by gestures and sign language. She has short upper arms and narrow shoulders and hips. A conspicuous delay in the eruption of the first deciduous teeth was seen. Her first teeth erupted at the age of 1.7 years (−6.2 SD) and at the age of 3.0 years her dental delay was −5.5 SD. She had slightly short ulnae and dysmorphic facial structures on x ray.
Patient IV (fig 2G, H) was born at 38+1 weeks' gestation and neonatally she had hypoglycaemia. She has suffered from gross feeding difficulties since birth and did not learn to suck properly until the age of 6 months. To this day she eats extremely small portions and her meals may take up to two hours. Her oral motor functions are normal. Her psychomotor development is somewhat delayed and she has a speech delay with articulation problems. At 2.6 years she spoke only in two to three word sentences with a soft voice. She has slight facial asymmetry with left side hypertrophy, small muscles including hypoplasia of the buttocks, a narrow pelvis, and her nails are weak and tend to chip on both hands and feet. She also has bilateral pes planovalgus, more severe on the right, and the long bones are slender onx ray. She has received growth hormone therapy from the age of 2.4 years onwards.
Comparison of the four matUPD(7) phenotypes with 28 non-matUPD(7) SRS patients suggests that matUPD(7) patients have a mild SRS phenotype and they may form a distinct clinical entity among SRS patients (fig 2, table 2). Facial triangularity was slight in the matUPD(7) patients in infancy and early childhood, whereas non-matUPD(7) patients showed distinctly triangular faces. MatUPD(7) patients had a broad and high forehead, low set and posteriorly rotated ears, relative macrocephaly, and craniofacial disproportion, which were equally seen in non-matUPD(7) patients. Micrognathia, a high arched or cleft palate, and downturned mouth corners are other classical SRS features that were seen in the vast majority of non-matUPD(7) patients, but those with matUPD(7) consistently lacked these features. Slight asymmetry of the lower limbs with concordant slight lower limb hemihypertrophy and facial asymmetry was seen in matUPD(7) patients I, II, and IV. Asymmetry and hemihypertrophy were also common, but both were more conspicuous in non-matUPD(7) SRS patients. Only two matUPD(7) patients had clinodactyly and brachydactyly of the fifth fingers but both were commonly seen in non-matUPD(7) SRS patients. Syndactyly of the second and third toes was also quite frequently observed in non-matUPD(7) SRS patients but was not present in the matUPD(7) patients. The matUPD(7) patients had a more sturdy appearance than the marked leanness typical of SRS patients (fig 2) and muscular hypoplasia was more frequently observed in non-matUPD(7) SRS patients (table 2). The growth patterns of matUPD(7) patients did not differ from non-matUPD(7) SRS patients (table 3). Both matUPD(7) and non-matUPD(7) SRS patients had an average delay in bone age of 1.6 years from their chronological ages. Growth hormone therapy has been administered to half of the matUPD(7) and SRS patients, and similar effects on growth were seen in both groups.
A varying degree of delayed development of the dentition was noted in matUPD(7) patients I-III (range −6.2 to −0.8 SD; dental examination was insufficient in patient IV) compared to SRS patients in general.30 Delayed emergence of the deciduous teeth was seen in all three and delayed development of the permanent teeth in patient I. Dental occlusion was of the class II type in all three, while in SRS patients class II was observed in only 14% (2/14) and class I type in the remaining 12/14.30 Cephalometric craniofacial measurements showed overall small dimensions, especially in patients II and III, with a very short posterior cranial base (<−3 SD) and total mandibular length (<−2 SD), as with SRS patients in general.30 The lower mandible of matUPD(7) patients was broader than generally observed in SRS patients and crowding of the lower incisors was only mild, distinguishing matUPD(7) from other SRS cases. In all three matUPD(7) patients the “hanging” posterior cranial fossa and the short cranial base were present with an abnormally anteriorly tilted foramen magnum and abnormal position of the first cervical vertebra. A short posterior cranial base, small mandible, and an abnormally tilted foramen magnum are commonly also seen in children with SRS, born SGA, and with growth hormone deficiency.31
All matUPD(7) patients suffered from excessive sweating and gross feeding difficulties, resulting from difficulties in sucking and swallowing and a lack of sense of hunger from birth onwards. Almost half of non-matUPD(7) SRS patients suffered from poor feeding in the first weeks of life, but matUPD(7) SRS patients still had extremely poor feeding at an average age of 3.4 years. Feeding difficulties have also been noted in four other matUPD(7) cases.6 19 23 Excessive sweating occurs in matUPD(7) patients shortly after falling asleep and after eating, but it was less frequently recorded in non-matUPD(7) SRS patients. Hypoglycaemic symptoms, such as fatigue and irritability, were not observed in any of our matUPD(7) patients. A history of feeding difficulties and excessive sweating is easily missed if the parents are not specifically asked about them. Therefore, the actual number of SRS patients with these symptoms might be much higher than reported.
MatUPD(7) patients tend to have more problems in development than non-matUPD(7) SRS patients. Neuropsychological developmental delay, predominantly in speech development, was recorded in all the matUPD(7) patients. All had problems in articulation and production of speech. The oldest patient I has difficulties in verbal skills and has received special education. Speech difficulties were only seldom observed in non-matUPD(7) SRS patients. Early motor developmental delay was also somewhat more prominent in matUPD(7) patients than in non-matUPD(7) SRS patients.
We thoroughly studied the phenotypes of four SRS matUPD(7) patients and found that they have a distinctly milder phenotype and share many common characteristics that distinguish them from the 28 non-matUPD(7) SRS patients. These matUPD(7) patients consistently lack the typical facial features of SRS and the dysmorphic facial features noted in matUPD(7) patients are in fact so minor, and progressively decrease with age, that their appearance might as well be regarded as normal. Previously reported matUPD(7) patients have also been noted to have a mild or incomplete SRS phenotype6 16 17 and even when SRS features were noted, they were described as only slight (triangular face, asymmetry of the limbs, and clinodactyly of the fifth digits) and typical features like micrognathia and downward slanting mouth corners were not noted in any matUPD(7) cases (table 2). The absence of a typical SRS facies in many of these previous matUPD(7) patients supports our finding that matUPD(7) patients do not present with a typical SRS face. Only 14/21 (67%) reported matUPD(7) cases have been diagnosed with SRS and it is possible that the dysmorphic findings in the very first reports of matUPD(7) cases were so mild that they were not observed or that they might be absent altogether.20-24 However, Spence et al 20 suspected that their patient might have SRS because of the observed body asymmetry. SRS features fade as children grow older and thus the diagnosis of SRS is easily missed in older children. In a recent study of 50 SRS patients attempting to set clinical criteria for SRS, a subgroup was observed presenting with homogeneous characteristics, including (1) classical dysmorphic facial features, (2) a higher frequency of asymmetry, (3) hand anomalies, (4) birth length below or equal to −2 SD from the mean, (5) poor postnatal growth below or equal to −2 SD from the mean, and (6) preservation of OFC.6 Patients included in this group generally had four of these criteria. No matUPD(7) cases fulfilled these criteria but they were noted to have a generally milder phenotype. Screening of matUPD(7) should therefore be focused on SRS patients with a mild phenotype and also on patients with severe intrauterine and postnatal growth retardation who do not clearly fulfil SRS criteria.
Interestingly, mild phenotypes have also been observed in UPD(15) patients compared to deletion patients. Angelman syndrome (AS) patients with patUPD(15) have consistently been observed to have a milder phenotype than AS cases with a deletion.32 33Prader-Willi syndrome (PWS) patients with matUPD(15) were found to have a face atypical of PWS more frequently than patients with a paternal deletion of chromosome 15q11-q13.34
We conclude that the uniformity of characteristics noted in four SRS patients with matUPD(7) raises the possibility that matUPD(7) patients might comprise a distinct phenotypic entity among SRS patients with a mild SRS phenotype. The characteristics distinctive of this subgroup include (1) pre- and postnatal growth retardation, (2) mild or absent SRS craniofacial dysmorphology consisting of slight or absent facial triangularity, no micrognathia, and no downturned mouth corners, (3) speech delay, (4) strikingly poor feeding throughout childhood, (5) excessive sweating without evidence of hypoglycaemic episodes, and (6) increased parental age at birth. The recent clinical findings of two matUPD(7) patients19 are consistent with the phenotypes of the four matUPD(7) cases described here, but thorough characterisation of other matUPD(7) cases is needed to verify these criteria. The delineation of possible subgroups among SRS cases would help in the clinical evaluation of SRS patients and also greatly facilitate the studies of the molecular aetiology of SRS, since genetic heterogeneity is widely postulated in SRS.
Acknowledgments
We would like to thank all of the families who participated in this study. Drs Ilkka Kaitila, Kalle Simola, and Hanna-Liisa Lenko are thanked for referring SRS patients. This study was supported by the P and S Sohlberg Foundation, Finnish Medical Foundation, Sigrid Juselius Foundation, Foundation for Paediatric Research, Ulla Hjelt Fund, Research and Science Foundation of Farmos, and the Academy of Finland.