Article Text

Statistics from Altmetric.com
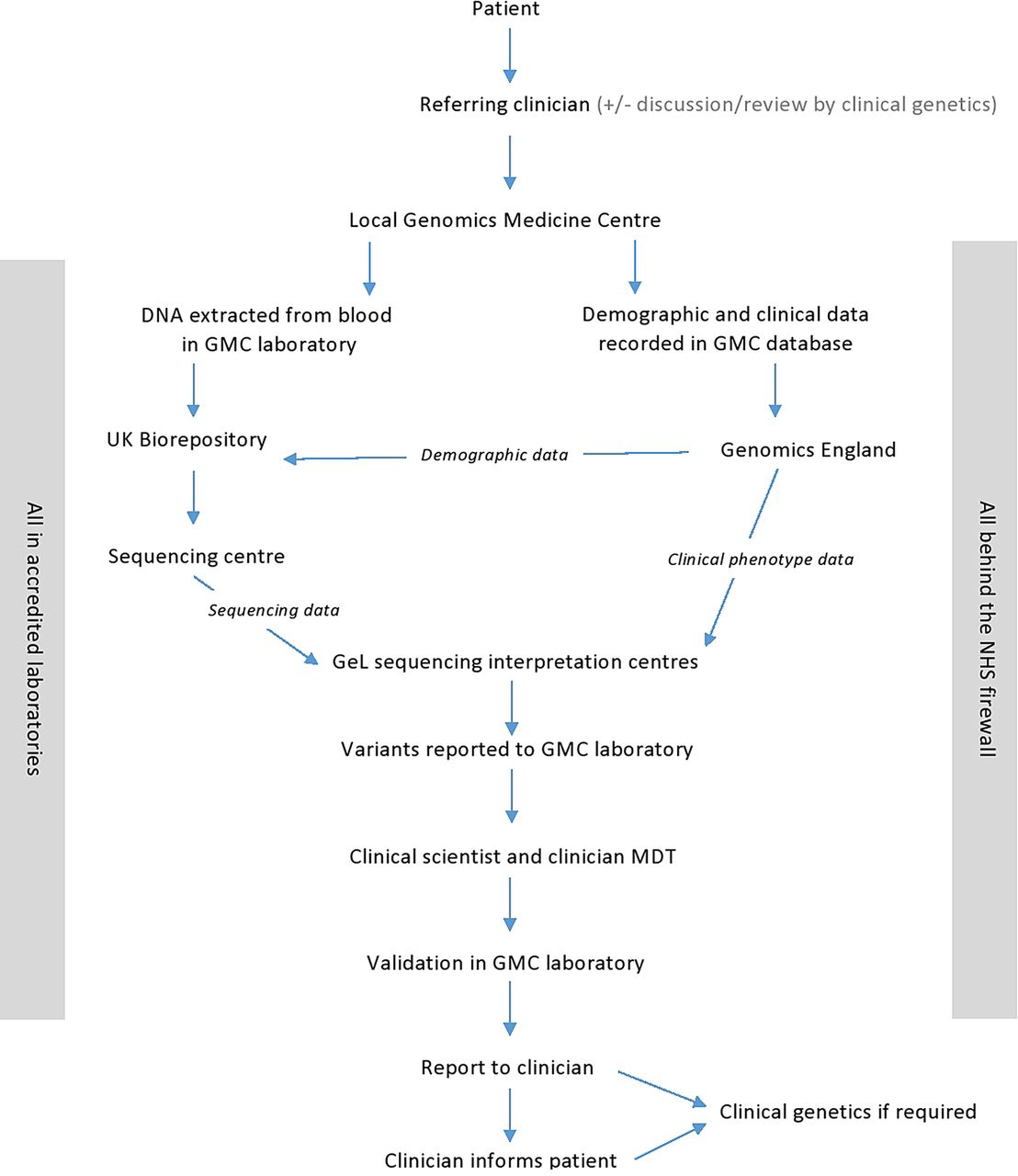
The 100 000 Genomes Project is a unique, national programme combining research and transformation of clinical care, by undertaking whole genome sequencing (WGS) in patients with rare diseases and cancer. Made possible by technological advances in next-generation sequencing1 and falling costs, this project aims to find the genes which cause a patient's rare disease and identify genetic changes which occur in the tumour of a child or adult with cancer, to understand the mechanism of disease and develop therapies to personalise treatment. Patients are recruited through the National Health Service (NHS) and their medical course is tracked for life through their NHS number with results fed back through routine NHS services. It will also lay the foundations for a new ‘genomic medicine’ service for the NHS.2 The project is coordinated by Genomics England, with participants enrolled through one of 13 NHS Genomic Medicine Centres (figure 1), covering all of England. Unlike genome projects in other countries3 that have yielded information on variants associated with common diseases and ancestry, the scale of the 100 000 Genomes Project is much greater. The ability to track long-term outcomes through the patients' NHS number provides a unique opportunity to link genomic and phenotypic data to hospital admissions (via hospital episode statistics) as well as lifelong response to interventions and treatments.

{kind=link}
Schema showing pathway from patient recruitment to results. Note the need for interaction between clinicians, scientists and geneticists working in multidisciplinary teams to deliver this new genomic medicine service. More detailed information can be found on the Genomics England website.2 GMC, Genomics Medicine Centre; GeL, Genomics England; MDT, multidisciplinary team meeting including clinical scientists, clinical geneticists and referring clinicians).
Which children are eligible and how to refer?
Many children with a rare disease but no known underlying cause are eligible. A local clinical geneticist4 or NHS Genomic Medicine Centre can advise on eligibility and recruitment. A detailed list and contact details can be found on the Genomics England website.5 Children with cancer who are undergoing biopsy or surgery are also eligible, with tumour and germline DNA sequenced in order to determine how the tumour arose and to target therapies. The Rare Diseases stream requires recruitment of several family members, usually the affected child and both parents, to facilitate interpretation of sequencing results and enable rapid exclusion of inherited non-pathogenic variants.
Who will benefit?
The main beneficiaries are children with rare diseases and their families as exemplified by the experience of one family who received a result recently (see box 1).6 Receiving a diagnosis puts an end to the ‘diagnostic odyssey’, potentially allows targeted treatment, and enables reproductive planning and offers opportunities to make contact with other families whose children have similar problems.7
Jessica's story
When Jessica was born, everything seemed fine but by the time she was a year old she was behind on all her milestones and at 13 months she had the first of many seizures. After many invasive tests, Jessica's parents were told that she had an undiagnosed condition. Her mother said: “It's the not knowing that I found really difficult. We spent hundreds of hours researching online and wondering ‘is it this terrible syndrome; is it that terrible syndrome?’”
They then heard about the 100 000 Genomes Project and consented to take part in the pilot study. Blood was taken from both Jessica and her parents so that changes in Jessica's genes could be compared with her parents' genomes. The sequencing results showed that Jessica had glucose transporter type 1 deficiency syndrome. At a public meeting of NHS Genomic Medicine Centre staff, her parents described some of the benefits the result had brought:
“Now that we have this diagnosis there are things that we can do differently almost straight away. Her condition is one that has a high chance of improvement on a special diet, which means that her medication dose is likely to decrease and her epilepsy may be more easily controlled. Hopefully she might have better balance so she can be more stable and walk more!”
“A diagnosis also means that we can link up with other families who are in the same boat and can offer support. The condition is still quite rare but there are definitely other children out there who have it. I'm really looking forward to saying ‘we are one of you; we have this problem too!”
“The results are also going to be very useful for family planning. If we had had another child before, we didn't know if they would certainly be affected by the same condition or if there was only a small chance. I think we can now say that there is only a tiny chance.”
“More than anything the outcome of the project has taken the uncertainty out for us and the worry of not knowing what was wrong. It has allowed us to feel like we can take control of things and make positive changes for Jessica.”
“It may also open doors to other research projects that we can to go on. These could be more specific to her condition and we are hopeful that they could one day find a cure.”
Unaffected family members may also benefit. During WGS many variants beyond those directly responsible for the primary condition can be identified. Specific ‘secondary’ findings can be fed back to adult participants, including information about conditions for which treatment or screening can be offered to detect disease at an early stage, for example, cancer predisposition genes and hypercholesterolaemia. Couples may also consent to receiving ‘reproductive findings’, for example, if both parents are identified as carriers for cystic fibrosis, they may opt in to having this information. Children will be reconsented when they are 16 years and can request details of secondary findings then.
This study will also stimulate biomedical research. Where a novel genetic cause of a rare disease is identified, validation and investigation to determine the disease mechanism is required. Where no obvious cause is found, further investigation may identify more subtle pathogenic findings. To facilitate this, research groupings called ‘Genomics England Clinical Interpretation Partnerships (GeCIPs)’ have been established; GeCIPs may be disease-specific or cross-cutting, to include ethics, social science research or population genomics. Commercial collaborations to develop new therapies and diagnostics are being established with several large pharmaceutical and biotechnology companies forming the GENE consortium.8 For both commercial and academic partners data security is high with all analysis performed in the secure data centre, sitting behind the NHS firewall using anonymised patient data.
What is the impact on paediatrics?
The impact on paediatrics will be profound. Diagnosis and implementation of targeted treatment for children will become more efficient. However, interpretation of findings from WGS requires multidisciplinary team efforts involving clinicians, clinical scientists and bioinformaticians, so healthcare professionals will need to work together to interpret and exploit this genomic information. Genomic medicine will become increasingly established in clinical practice, but the manpower and skills required cannot be met within current clinical genetics services. The 100 000 Genomes Project will become a training ground to establish patterns of working that include general and specialist paediatricians working together with clinical scientists. We need to train a new generation of healthcare professionals in genomic medicine, and existing clinicians need support as they come to grips with genomic medicine. Primary and secondary findings from WGS will need to be communicated to patients and families in a manner that is effective, appropriate and achievable. Health Education England is leading the delivery of education in genomics across the healthcare sector as part of the 100 000 Genomes Project, offering a wide range of courses from a Masters in Genomic Medicine and CPD modules to online courses and brief aids to understanding all aspects of WGS.9
Conclusions
Technical challenges of WGS are being overcome, but ethical ones remain. What findings should be returned? How to ensure patients give informed consent? Should results be reviewed longitudinally as knowledge improves? If so how? Maybe the biggest immediate challenge is educating our workforce to deliver this exciting new technology. Changes to clinical practice will be far-reaching. More than ever we will need to work in multidisciplinary teams to enable accurate diagnosis and deliver appropriate therapy. These are exciting times, both for patients who are recipients of this new technology, but also for health professionals using it as part of their clinical armamentarium.
Earlier this year, the parents of the first two children to receive feedback from the 100 000 Genomes Pilot study spoke publicly about the impact of finally receiving a diagnosis (see box 1). These families and their healthcare teams had been struggling for years to identify the cause of their child's problems. The profound and positive effect this had on the families was summed up by one mother “When they said that they'd found something it was one of the biggest days of my life.”
Footnotes
Competing interests None declared.
Provenance and peer review Commissioned; externally peer reviewed.