Article Text

Abstract
Advances in technology have led to a massive expansion in the capacity for genomic analysis, with a commensurate fall in costs. The clinical indications for genomic testing have evolved markedly; the volume of clinical sequencing has increased dramatically; and the range of clinical professionals involved in the process has broadened. There is general acceptance that our early dichotomous paradigms of variants being pathogenic–high risk and benign–no risk are overly simplistic. There is increasing recognition that the clinical interpretation of genomic data requires significant expertise in disease–gene-variant associations specific to each disease area. Inaccurate interpretation can lead to clinical mismanagement, inconsistent information within families and misdirection of resources. It is for this reason that ‘national subspecialist multidisciplinary meetings’ (MDMs) for genomic interpretation have been articulated as key for the new NHS Genomic Medicine Service, of which Cancer Variant Interpretation Group UK (CanVIG-UK) is an early exemplar. CanVIG-UK was established in 2017 and now has >100 UK members, including at least one clinical diagnostic scientist and one clinical cancer geneticist from each of the 25 regional molecular genetics laboratories of the UK and Ireland. Through CanVIG-UK, we have established national consensus around variant interpretation for cancer susceptibility genes via monthly national teleconferenced MDMs and collaborative data sharing using a secure online portal. We describe here the activities of CanVIG-UK, including exemplar outputs and feedback from the membership.
- genetics
- clinical genetics
- guidelines
- molecular genetics
- oncology
This is an open access article distributed in accordance with the Creative Commons Attribution 4.0 Unported (CC BY 4.0) license, which permits others to copy, redistribute, remix, transform and build upon this work for any purpose, provided the original work is properly cited, a link to the licence is given, and indication of whether changes were made. See: https://creativecommons.org/licenses/by/4.0/.
Statistics from Altmetric.com
Background
Clinical utility of cancer susceptibility genes (CSGs)
Analysis of germline (constitutional) variants in CSGs constitutes approximately one-quarter of activity in NHS Molecular Diagnostic Laboratories in England.1 Following identification of a pathogenic variant (PV) in a CSG, incidence of/mortality from future cancers may be mitigated via (1) risk-reducing surgery (eg, mastectomy, gastrectomy, salpingo-ophorectomy and colectomy); (2) chemoprevention; (3) intensive screening; and (4) lifestyle modification.2 Family members negative for the familial CSG-PV can be spared anxiety and unnecessary screening. Many CSGs are associated with a pattern of cancer risk that is late-onset, variably penetrant and of autosomal dominant inheritance. PV-positive family members identified via cascade screening are often distributed across disparate genomics services.
Erroneous interpretation of CSG variant pathogenicity can therefore result in (1) discordant management within families, (2) serious clinical consequences for individuals and (3) misdirection at population level of resources for screening and prevention.3–5 Increasingly, CSG-PVs are used as predictive biomarkers to inform cancer therapy. For all these reasons, robust, rapid, accurate variant analysis and interpretation of disease risk are critical to effective delivery of germline cancer genetics and improving outcomes for patients.
Evolving landscape of variant interpretation in germline cancer genetics
In the late 1990s, within a few years of identification of the relevant genes, laboratory analysis of CSGs became available in the UK via family cancer clinics.2 If the cancer phenotype ascribed to the gene matched that found in the proband/family under study, with little additional evidence, a rare variant would often be labelled as pathogenic and thus causative.6 Subsequent large-scale population sequencing studies have revealed the degree of innocuous variation present in the human genome (and indeed in disease-associated genes) and ‘downgrading’ of many erroneously labelled PVs has been required.7 An era of caution followed, with much greater recourse to labelling of variants as ‘variants of uncertain significance’ (VUS/VOUS). However, lack of systems for sharing new evidence has meant that many families have spent years in limbo with their ‘VUS’, even when data had long been available by which classification of their variant could be downgraded or upgraded.
Sharing of clinical variant data was somewhat improved with the advent of locus-specific databases (LSDs), such as Breast Cancer Information Core and Leiden Open Variant Databases.8–11 However, the curation of clinical and molecular data in LSDs often remains suboptimal, with (1) erroneous nomenclature, (2) duplication of entries and (3) use of differing classification systems resulting in contradictory assignations.12
Using Myriad Genetics data from ~70 000 genetic tests for hereditary breast and ovarian cancer, in 2007, Easton and colleagues published a landmark multifactorial analysis through which ‘odds of causality’ were mathematically generated for 1433 variants using clinical, pedigree and allelic data.13 In 2008, International Agency for Research on Cancer (IARC) collaborators published the first formal five point variant interpretation system for CSGs, which included numeric thresholds for the probability of pathogenicity.14 Expert cancer susceptibility consortia such as the Evidence-based Network for the Interpretation of Germline Mutant Alleles (ENIGMA) and the International Society for Gastrointestinal Hereditary Tumours (InSIGHT) further evolved these multifactorial variant classification systems to incorporate tumour phenotype and in silico predictions.15–17 However, ENIGMA/InSIGHT approaches require statistical genetic–epidemiological analyses of large curated data series and are not reproducible by an individual diagnostic laboratory seeking to classify in a clinically relevant timescale a newly identified variant.
In 2015, the American College of Medical Geneticists (ACMG) published a variant interpretation framework enabling the combination by a diagnostic laboratory of disparate evidence sources for a newly identified genomic variant.18 The ACMG framework has subsequently been further evolved under the auspices of ClinGen, including (1) specification for how it is applied to particular genes and/or diseases (including TP53, CDH1 and PTEN); (2) deeper specification of particular criteria (eg, functional assays); and (3) exposition of the underpinning Bayesian model.19–23
Coordinated national UK approaches in variant interpretation
In 2016, with endorsement from NHS England and Health Education England, it was agreed formally by the UK Association of Clinical Genomic Science (UK-ACGS) to adopt the ACMG variant interpretation framework.24 25 The UK-ACGS established national groups for rare disease, germline cancer genetics, cardiac disease and hypercholesterolaemia to develop and disseminate practice in the application of the ACMG variant interpretation framework.24 In parallel was recognition within the NHS Genomic Medicine Service of the need for national subspecialist genomics MDMs.26 27 In response to these dual recommendations, Cancer Variant Interpretation Group UK (CanVIG-UK) was initiated in 2017.
Cancer Variant Interpretation Group UK
The purpose of CanVIG-UK is to advance outcomes for patients by improving the accuracy and consistency of interpretation of variants in CSGs across the UK clinical genetics and molecular diagnostic laboratory communities (hereafter termed the UK clinical-laboratory community). We aim to progress this goal by advancing six objectives (see box 1).
CanVIG Objectives
The purpose of Cancer Variant Interpretation Group UK (CanVIG-UK) is to advance outcomes for patients by improving the accuracy and consistency of interpretation of variants in Cancer Susceptibility genes across the UK clinical-laboratory community. We have six specific objectives:
Creation of a national multidisciplinary professional network and regular forum.
Training and education.
Detailed specification for germline cancer genetics of the UK-ACGS Best Practice Guidelines for Variant Interpretation.
Ratification of additional guidance in germline cancer genetics relevant to the UK clinical-laboratory community.
Development of an online platform to facilitate information sharing and variant interpretation within the UK clinical-laboratory community.
UK contribution to international variant interpretation endeavours.
Creation of a national multidisciplinary professional network and regular forum
CanVIG-UK has grown to now include >100 members, incorporating clinical and laboratory representation from each of the 25 Molecular Diagnostic Laboratories and Clinical Genetics Services of the UK (NHS) and Ireland (see collaborators). This group comprises roughly equal proportions of clinical scientists and clinical geneticists, with two-thirds working exclusively or predominantly in cancer genetics (figure 1):

Overview of the CanVIG-UK membership profile (survey of CanVIG-UK members, performed on 29 October 2019, return rate 83/103 (81%). HBOC, hereditary breast and ovarian cancer; MMR, mismatch repair. CanVIG-UK, Cancer Variant Interpretation Group UK.
The monthly teleconferenced MDM provides a forum to which problematic variants/cases are submitted. The variants submitted to the monthly variant surgery are circulated 1 week in advance. CanVIG-UK members are asked (1) to ascertain whether additional cases and/or laboratory data exist locally and (2) to undertake local, independent classification of the variant. The relevant clinical and laboratory data are presented by the nominating laboratory. This is followed by input of any additional information by the broader CanVIG-UK group and a discussion regarding the legitimacy of the ACMG criteria awarded. Following this discussion and an online postdiscussion poll, a consensus CanVIG classification is generated (see online supplementary table 1). A detailed date-stamped CanVIG variant summary sheet is generated (see online supplementary appendix 2), which is circulated by email, uploaded to the CanVar-UK portal and submitted to ClinVar.
The CanVIG-UK network is active throughout the month via the email forum, through which urgent queries can be debated and addressed.
Supplemental material
Supplemental material
Training and education
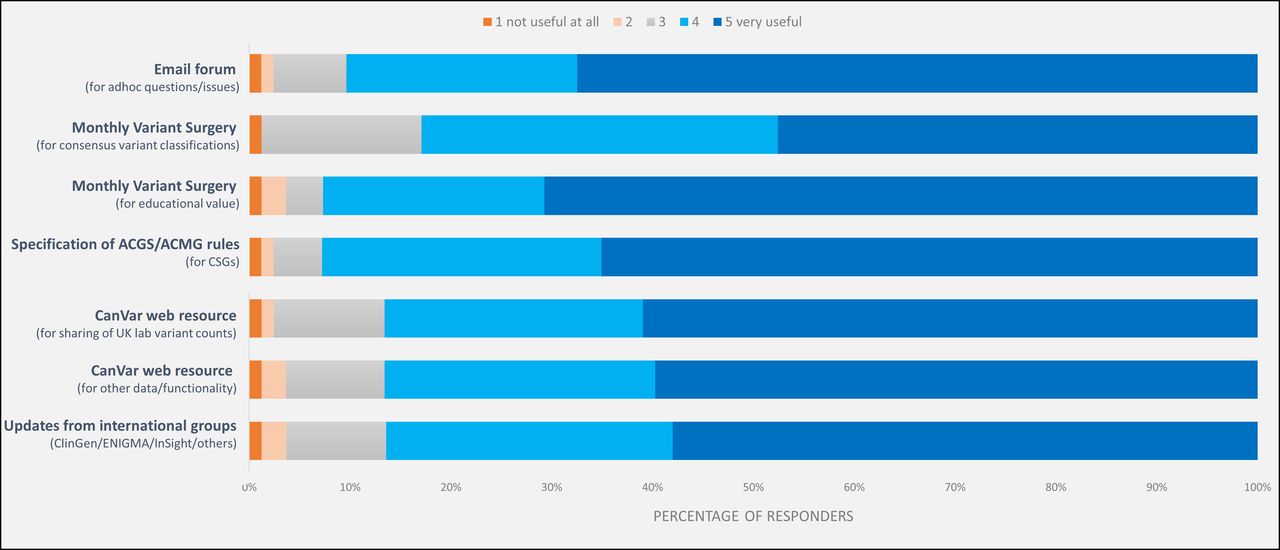
The discussion of cases at the MDM also provides valuable education for the clinical-laboratory community regarding application of the ACMG framework and the vagaries of the evidence sources used (see figure 2). Additionally, through CanVIG-UK, we have supported training of the broader UK genetics and oncology communities in variant interpretation for CSGs.

{kind=link}
{kind=link}
Perceived utility of CanVIG-UK activities regarding local practice in CSG variant interpretation of seven activities (5: very useful to 1: not useful; survey of CanVIG-UK members, performed on 29 October 2019, return rate 83/103 (81%)). ACGS, Association of Clinical Genomic Science; ACMG, American College of Medical Geneticists; CanVIG-UK, Cancer Variant Interpretation Group UK; CSG, cancer susceptibility gene.
Detailed specification for germline cancer genetics of the UK-ACGS Best Practice Guidelines for Variant Interpretation
On behalf of the UK-ACGS, the rare disease variant interpretation group has generated and updates annually a highly detailed specification of the ACMG variant interpretation framework .24 In cancer susceptibility, we typically observe variants relating to late-onset, common phenotypes. De novo and biallelic paradigms are infrequent. We are typically much more reliant on variant frequency from case series and functional assays. Thus, an important remit for CanVIG-UK has been to develop a detailed specification of the UK-ACGS framework for these types of evidence to be used for CSG variant interpretation (see online supplementary appendix 1).
Ratification of additional guidance in germline cancer genetics relevant to the UK clinical-laboratory community
Historically, the first presentation to the family cancer clinic was typically an unaffected individual, concerned by a significant family history. Increasingly, genetic analysis is now performed as part of routine work-up at cancer diagnosis, either through analysis of a germline sample or through therapeutically motivated molecular analysis of the tumour. In both contexts, (1) focused testing of one or two genes has often been superseded by broad ‘cancer panels’ containing dozens or hundreds of genes; (2) patients may be unselected for family history; and (3) analysis and reporting in a tight time frame is typically required. A number of challenging issues have emerged, including
Categorisation and management of reduced penetrance variants in high-penetrance genes.
Variant interpretation and clinical management for moderate-penetrance genes.
Adaptation of variant interpretation and risk for different contexts of ascertainment.
Inference of germline findings from tumour-only sequencing.
While germane across genomics, consideration of these issues has become pressing within germline cancer genetics. Benefitting from its regular forum, multidisciplinary membership and alignment with both UK-ACGS and the UK Cancer Genetics Group (UK-CGG), we have used the CanVIG–UK monthly forum to evolve UK national multidisciplinary approaches on such issues (see online supplementary appendix 3).
Development of an online platform to facilitate information sharing and variant interpretation within the UK clinical-laboratory community
In germline cancer genetics, enrichment in cases (especially ‘strong families’) is one of the most valuable clinical observations indicating variant pathogenicity. However, to date, we have struggled to quantify such observations on account of (1) failure to aggregate national data from distributed laboratories and (2) lack of a robust denominator.
In a collaborative venture between Public Health England (PHE) and the national network of molecular diagnostic laboratories, data from molecular testing of CSGs have been submitted via a pseudonymisation portal to the secure National Cancer Registration and Analysis Service (NCRAS) data environment of PHE.28 The national variant totals (numerator and denominator) are then shared by CanVIG-UK with the UK clinical-laboratory community via our online data system CanVar-UK (http://www.canvaruk.org/).
CanVar-UK provides additional annotations for 1 008 643 variants from 95 CSGs. It includes variant-level annotations from LSDs (case counts), functional assays, splicing assays and multifactorial analyses for selected genes. Accessible only to registered CanVIG-UK clinical-laboratory users is a community area for sharing non-identifiable variant-level data, such as local classifications, comments/notes, uploaded documents and results from local laboratory assays (eg, RNA analyses of potential splicing variants).
UK contribution to international variant interpretation endeavours
CanVIG-UK is an effective conduit between the UK clinical-laboratory germline cancer genetics community and relevant international variant interpretation endeavours in several regards:
First, there is representation at the international ClinGen SVI group from the leadership of the UK-ACGS rare disease variant interpretation group. The regular crosstalk between leadership of the UK groups enables appraisal of the ClinGen SVI group of emerging analyses and activity within CanVIG-UK and the UK clinical-laboratory cancer genetics community.
Second, multiple members of CanVIG-UK are members of gene-specific international endeavours such as ENIGMA, InSIGHT and ClinGen expert groups.
Third, data generated by CanVIG-UK data have contributed to collaborative international consortia analyses, for example, provision to ENIGMA of the summary PHE UK laboratory data on BRCA1/BRCA2 variants.
Fourth, CanVIG-UK consensus classifications (and underpinning evidence) are shared via ClinVar. CanVIG-UK is the first UK organisation to submit clinical-laboratory variant classifications to ClinVar.
Sustainability
Maintenance of a national multidisciplinary network, coordination of a regular teleconferenced MDMs and development of a data system is only feasible via sustained support. The activities of CanVIG-UK are currently supported by a Cancer Research UK Catalyst Award (CanGene-CanVar, @CangeneCanvar, C61296/A27223).
Conclusion
CanVIG-UK is a multidisciplinary group comprising >100 clinical scientists and senior genetics clinicians working in germline cancer genetics, with representation from across the 25 NHS molecular diagnostic laboratories of the UK and Ireland. Through CanVIG-UK, the UK clinical-laboratory germline cancer genetics community have evolved:
An email forum for real-time consultation on problematic variants.
A monthly teleconferenced MDM for detailed review of challenging variants and cases.
A national programme of using secure submissions of frequency data from PHE.
An online data system (CanVar-UK) for sharing variant-level data both publicly and within a secure community region.
Detailed, consensus UK guidance for the interpretation of variants in CSGs.
Fruitful interactions with international CSG variant interpretation endeavours.
In summary, we propose CanVIG-UK as an exemplar National Subspecialty Multidisciplinary Genomics Network. In this era of rapid emergence of genomic knowledge, such networks are becoming increasingly important to optimise collaborative specialist case review, information sharing and education.
Acknowledgments
We acknowledge the contribution of Jenny Lord and Andrew Douglas to discussions regarding splicing guidance.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @BurghelG, @LaughingGenome, @ER_Woodward, @clare_turnbull
AG, AC and MD contributed equally.
Collaborators CanVIG-UK: Stephen Abbs, Patrick Tarpey, Jonathan Bruty, James Drummond, James Whitworth, Anne Ramsay Bowden, Marc Tischowitz, Eamonn Maher (Cambridge University Hospitals NHS Foundation Trust); Shirley Heggarty, Sean Hegarty, Rosalind Martin, Peter Logan, Claire Byrne (Belfast Health and Social Care Trust); Yvonne Wallis, Samantha Butler, Rachel Hart, Lowri Hughes, Kim Reay, Kai-Ren Ong, Joanne Mason, Ian Tomlinson (Birmingham Women's and Children's NHS Foundation Trust); Ian Frayling, Sheila Palmer-Smith, Julian Sampson, Alex Murray (Cardiff and Vale University Health Board); Munaza Ahmed, Louise Kiely, Louise Busby, Claire Brooks, Alison Taylor-Beadling, Ajith Kumar (Great Ormond Street Hospital for Children NHS Foundation Trust); Vishakha Tripathi, Mina Ryten, Louise Izatt, Anjana Kulkarni, Adam Shaw, Joanna Campbell (Guy's and St Thomas' NHS Foundation Trust); Huw Thomas (St. Mark's Hospital, Northwick Park Hospital, Harrow); Daniel Chubb, Mary Alikian, Cankut Cubuk (Institute of Cancer Research); Rachel Robinson, Brendan Mullaney, Julian Adlard (Leeds Teaching Hospitals NHS Trust); Karen-Lynn Greenhalgh, Emma Howard (Liverpool Women’s NHS Foundation Trust); Virginia Clowes, Angela Brady (London North West University Healthcare NHS Trust); George Burghel, Emma Woodward, Philip T Smith, Jade L Harris, Naomi L Bowers, Claire L Hartley, Ronnie Wright, Gareth Evans, Fiona Lalloo, Andrew Wallace (Manchester University NHS Foundation Trust); John Burn, James Tellez, Sarah Mackenzie, Helen Powell (Newcastle Upon Tyne Hospitals NHS Foundation Trust); Stephen Tennant, Joanna Tolmie, Dawn O'Sullivan (NHS Grampian, Aberdeen); Rosemarie Davidson, Jonathan Grant, Daniel Stobo, Aisha Ansari (NHS Greater Glasgow & Clyde); Jennie Murray, David Moore (NHS Lothian, Edinburgh); Rachael Tredwell, Joanne Field, Kirsty Bradshaw, Rachel Harrison (Nottingham University Hospital NHS Trust); Logan Walker (University of Otago, Christchurch, New Zealand); Trudi Mcdevitt, Marie Duff, Catherine Clabby (Our Lady's Children's Hospital, Crumlin, Dublin); Treena Cranston, Tina Bedenham, Evgenia Petrides, Lara Hawkes (Oxford University Hospitals NHS Foundation Trust); Fiona McRonald (Public Health England); Sian Ellard, Ruth Cleaver, Carole Brewer (Royal Devon And Exeter NHS Foundation Trust); Nick Woodwaer (Royal Free London NHS Foundation Trust); Stacey Daniels, Alison Callaway (Salisbury NHS Foundation Trust); Khalid Tobal, Shadi Albaba, Sarah Dell, Rodney Nyanhete, Richard Kirk, Mark Watson, Miranda Durkie, Jackie Cook, Hazel Clouston, Anne-Cecile Hogg (Sheffield Children's NHS Foundation Trust); Sabrina Talukdar, Lorraine Hawkes, Laura Cobbold, Kate Tatton-Brown, Helen Hanson, Katie Snape, Charlene Crosby, Ayaovi Hadonou Juan Carlos Del Rey Jimenez(St George's University Hospitals NHS Foundation Trust); Zoe Kemp, Terri Mcveigh, Clare Turnbull, Alice Garrett (The Royal Marsden NHS Foundation Trust); Cathal O'Brien (Trinity College Dublin, The University Of Dublin, Ireland); Laura Yarram, Kenneth Smith, Helen Williamson, Alan Donaldson (University Hospitals Bristol NHS Foundation Trust); Julian Barwell (University Hospitals of Leicester NHS Trust); Matilda Bradford (University Hospitals Plymouth NHS Trust); Lucy Side, Diana Eccles, Diana Baralle, Anneke Lucassen (University Hospital Southampton NHS Foundation Trust).
Contributors The manuscript was drafted by CT, AG, AC and MD. All other authors contributed to the final manuscript.
Funding This work is supported by the CRUK Catalyst Award CanGene-CanVar (C61296/A27223). ERW and DGE are supported by the Manchester National Institute for Health Research Biomedical Research Centre (IS-BRC-1215- 20007).
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.