Article Text

Abstract
The main objective of this study was to perform a systematic review and meta-analysis on the risk of developing malignant paraganglioma (PGL) in SDHB-mutation and SDHD-mutation carriers. PubMed, EMBASE, Web of Science, COCHRANE and Academic Search Premier (2000–August 2011) and references of key articles were searched to identify potentially relevant studies. The main outcomes were the pooled incidence and prevalence of malignant PGL in SDHB-mutation and SDHD-mutation carriers. A meta-analysis was performed with an exact likelihood approach using a logistic regression with a random effect at the study level. Twelve studies were included. The pooled incidence of malignant PGL in populations comprising both asymptomatic mutation carriers and mutation carriers with manifest non-malignant PGL was 17% (95% CI 10 to 28) for SDHB-mutation carriers and 8% (95% CI 2 to 26) for SDHD-mutation carriers. The pooled risk in prevalence studies was 13% (95% CI 4 to 34) and 4% (95% CI 2 to 7), respectively. In studies comprising only mutation carriers with manifest disease, the pooled prevalence was 23% (95% CI 16 to 33) for SDHB-mutation and 3% (95% CI 1 to 10) for SDHD-mutation carriers. Incidence and prevalence of malignant PGL are higher in SDHB-mutation than in SDHD-mutation carriers, but lower in SDHB-mutation carriers than hitherto appreciated.
- Cancer: endocrine
- Clinical genetics
- Genetic screening/counselling
Statistics from Altmetric.com
Introduction
Background
Paragangliomas (PGLs) are rare tumours of paraganglia which are neural-crest derived chromaffin tissues, associated with the autonomic nervous system. In general, PGLs of the head and neck region (HNPGLs) are neoplasms of the parasympathetic part of the autonomous nervous system, while adrenal PGLs (also termed pheochromocytomas) and extra-adrenal non-HNPGLS are neoplasms of the sympathetic nervous system.
PGLs can occur sporadically or as part of a hereditary syndrome (ie, familial PGL, von Hippel-Lindau disease, multiple endocrine neoplasia type 2 or neurofibromatosis type 1).1–5 Familial PGL is associated with germline mutations in subunits A, B, C, D or assembly factor 2 of the mitochondrial complex II-succinate dehydrogenase (SDH) gene, which encodes Krebs cycle proteins.4 ,6–10 Mutations in subunits A, C and assembly factor 2 appear to be more rare than mutations in subunits B or D.4 ,8 ,11–13
SDHB-mutations are more frequently associated with pheochromocytomas, extra-adrenal non-HNPGLS and malignant disease, than mutations in one of the other subunits of the SDH gene. SDHD-mutation carriers typically present with multifocal HNPGLs, although they also may develop malignant PGLs.14–16 The actual risk of developing malignant PGL in SDHB-mutation and SDHD-mutation carriers is subject of debate. Reported proportions of malignant PGL vary considerably between most genotype–phenotype studies, ranging from 31% to 71.4% in SDHB-mutation carriers and from 0% to 22.7% in SDHD-mutation carriers.1 ,11 ,15 ,17 ,18 Most articles concern cross-sectional studies of patients, treated in tertiary care referral centres, hence, referral bias may lead to an overestimation of these proportions. Consequently, giving an exact estimate for the proportion of patients developing malignant PGL is difficult.
To date, an increasing number of SDHB-mutation and SDHD-mutation carriers are identified through molecular genetic testing of family members of PGL-patients with manifest disease, that is, index cases. It is important to be able to provide newly identified mutation carriers with accurate prognostic information, including their risk of developing malignant PGL. Therefore, a more accurate estimation of the risk of malignant PGL in SDHB-mutation and SDHD-mutation carriers is warranted.
Objective of the study
To date, no systematic review has been published giving an overview of the risk of developing malignant PGLs in SDHB-mutation and SDHD-mutation carriers. The aim of the present systematic review and meta-analysis is to assess the incidence and prevalence of malignant disease, stratified by mutation and disease status (mutation carriers with and without manifest disease).
Materials and methods
Eligibility criteria
Studies assessing the incidence (ie, follow-up studies) or prevalence (ie, cross-sectional studies) of malignant PGL in SDHB-mutation or SDHD-mutation carriers were eligible for inclusion. Both studies concerning asymptomatic mutation carriers at baseline, and studies concerning patients with manifest non-malignant PGL due to SDHB-mutations or SDHD-mutations, were considered for inclusion. Studies including patients with PGLs without molecular genetic testing for SDHB-mutations or SDHD-mutations were not eligible.
We set out to analyse the proportion of patients with malignant PGLs among mutation carriers. Since there are no reliable histologic features to distinguish benign from malignant PGLs, malignant disease is generally defined as the presence of metastases, that is, the presence of chromaffin tissue in non-chromaffin organs or tissues, distant from the primary tumour.19–21 Only studies using this definition were eligible for inclusion.
As the aim of our meta-analysis was to determine the incidence and prevalence of metastatic PGLs in SDHB-mutation and SDHD-mutation carriers, studies including patients who were tested for these mutations because of the presence of malignant disease were not included, the reason being that inclusion of such studies would result in an overestimation of the risk estimate due to selection bias. If it was unclear whether patients were tested because of malignant disease, the study was included, but was classified as having a high risk of bias.
In case of multiple studies describing the same cohort of patients, only the study which comprised the highest number of subjects and/or the longest duration of follow-up was included for this review. Furthermore, only studies comprising a population of more than 10 SDHB-mutation or SDHD-mutation carriers were included. Eligible studies were restricted to languages familiar to the authors (English, French, German and Dutch).
Search strategy
In August 2011, PubMed, EMBASE, Web of Science, COCHRANE and Academic Search Premier were searched to identify potentially relevant studies (see appendix 1, supplementary material). References of key articles were assessed for additional relevant articles. The search was limited to studies published from 2000 onwards, since this was the first year with publications on SDHD-mutations in PGL.7 The first study on SDHB-mutations in PGL was published in 2001.6
Data extraction
All studies obtained from the search strategy were entered into reference manager software (Reference Manager V.12) and were screened on title and abstract. Potentially relevant studies were retrieved for detailed assessment. For eligible studies, data were independently extracted by two reviewers (LvH and EC). Disagreements between reviewers were resolved by consensus, but when doubt remained, a third reviewer (OD) decided.
For all included studies, the following data were extracted and entered into an electronic database: first author, year of publication, study design, setting (eg, referral centre), population studied, number of subjects with proven SDHB-mutation or SDHD-mutation, mean age, number of subjects with SDHB-mutation or SDHD-mutations analysed for malignant PGL, duration of follow-up, number of subjects lost to follow-up, and reason for loss to follow-up. Studies were classified as either a cohort (follow-up) study or a cross-sectional study.22 ,23
Incidence and prevalence of metastatic disease
The incidence of metastatic disease was calculated as the number of new cases divided by the number of patients with a mutation followed over time. In principle, only mutation carriers initially free of the outcome (metastatic disease) and followed over time, could contribute to the incidence.
The prevalence of metastatic disease was calculated as the number of cases with metastatic disease divided by the number of screened mutation carriers. Reliable prevalence estimation requires that mutation carriers are not tested for the mutation because of the presence of metastatic disease. Such selection bias leads to an overestimation of the prevalence. Whenever possible, we extracted data on metastatic disease only for mutation carriers not sampled on the outcome.
We aimed to assess the incidence and prevalence of metastatic disease separately for mutation carriers with manifest PGLs, and mutation carriers who were asymptomatic at time of entering the study. Since mutation carriers with a manifest PGL have already proven to be able to develop an SDH-related disease, the risk for malignant SDH manifestations may differ for carriers with and without manifest disease.
Risk of bias assessment
The present meta-analysis is based on observational studies. Risk of bias assessment was based on design elements that potentially bias an association between the mutation (SDHB or SDHD) and the outcome (malignant PGL):
-
Adequacy of exposure (SDHB-mutation or SDHD-mutation) determination. A clearly described method of germline mutation detection in the coding exons of SDHB and/or SDHD was considered an adequate exposure determination.
-
Adequacy of definition and assessment of malignant PGL. As described above, the presence of metastases was considered an adequate definition of malignant PGL. Performance of anatomical imaging (CT scanning and/or MRI scanning), electively combined with functional imaging (ie, 123I metaiodobenzylguanidine (MIBG) scintigraphy, octreotide scintigraphy or 18F-3,4-dihydroxyphenylalanine positron emission tomography (DOPA PET)), or histological proof of metastases of PGL was considered an adequate assessment of malignant PGL.
-
Selection of patients. Inclusion of consecutive exposed patients or a random sample of the inception cohort with exposure unrelated to the outcome was considered adequate.
-
For incidence estimation: adequacy of follow-up. A proportion of loss to follow-up <10% was considered adequate.
Elements of risk of bias assessment were used to explore potential heterogeneity.
Statistical analysis
The main outcome of the present meta-analysis was the pooled incidence and prevalence of PGL-related malignant disease, that is, metastatic disease, in SDHB-mutation and SDHD-mutation carriers. For all studies, the proportion of patients with metastatic disease was calculated as the number of patients with metastatic disease divided by the total number of SDHB-mutation or SDHD-mutation carriers analysed for malignant PGL. For all proportions, exact 95% CIs were calculated.
Meta-analysis was performed using an exact likelihood approach. The method used was a logistic regression with a random effect at the study level. Given the expected clinical heterogeneity, a random effects model was performed by default and no fixed-effects analyses were performed. For meta-analysis of proportions, the exact likelihood approach based on a binomial distribution has advantages compared with a standard (DerSimonian and Laird) random effects model that is based on normal distributions. First, estimates from a binomial model are less biased than estimates from models based on a normal approximation. This is especially the case for proportions that are close to 0 or 1. Second, no assumptions are needed for the exact approximation when dealing with zero-cells, whereas, the standard approach needs to add an arbitrary value (often 0.5) when dealing with zero-cells. Adding values to zero-cells is known to contribute to the biased estimate of the model. All analyses were performed with STATA 12.0 (Stata Corp, Texas, USA).
Results
Study selection
The initial search resulted in 275 unique records; 38 were selected for detailed assessment (figure 1). After detailed assessment, 26 articles were excluded. Six articles were excluded for the following reasons: no description of the number of patients with malignancies (n=1),24 no stratification of patients with malignancies per mutation (n=2),25 ,26 lack of original data (n=3).27–29 Seven articles were not eligible for inclusion because studied cohorts included patients with already diagnosed malignant PGL.1 ,11 ,16 ,30–33
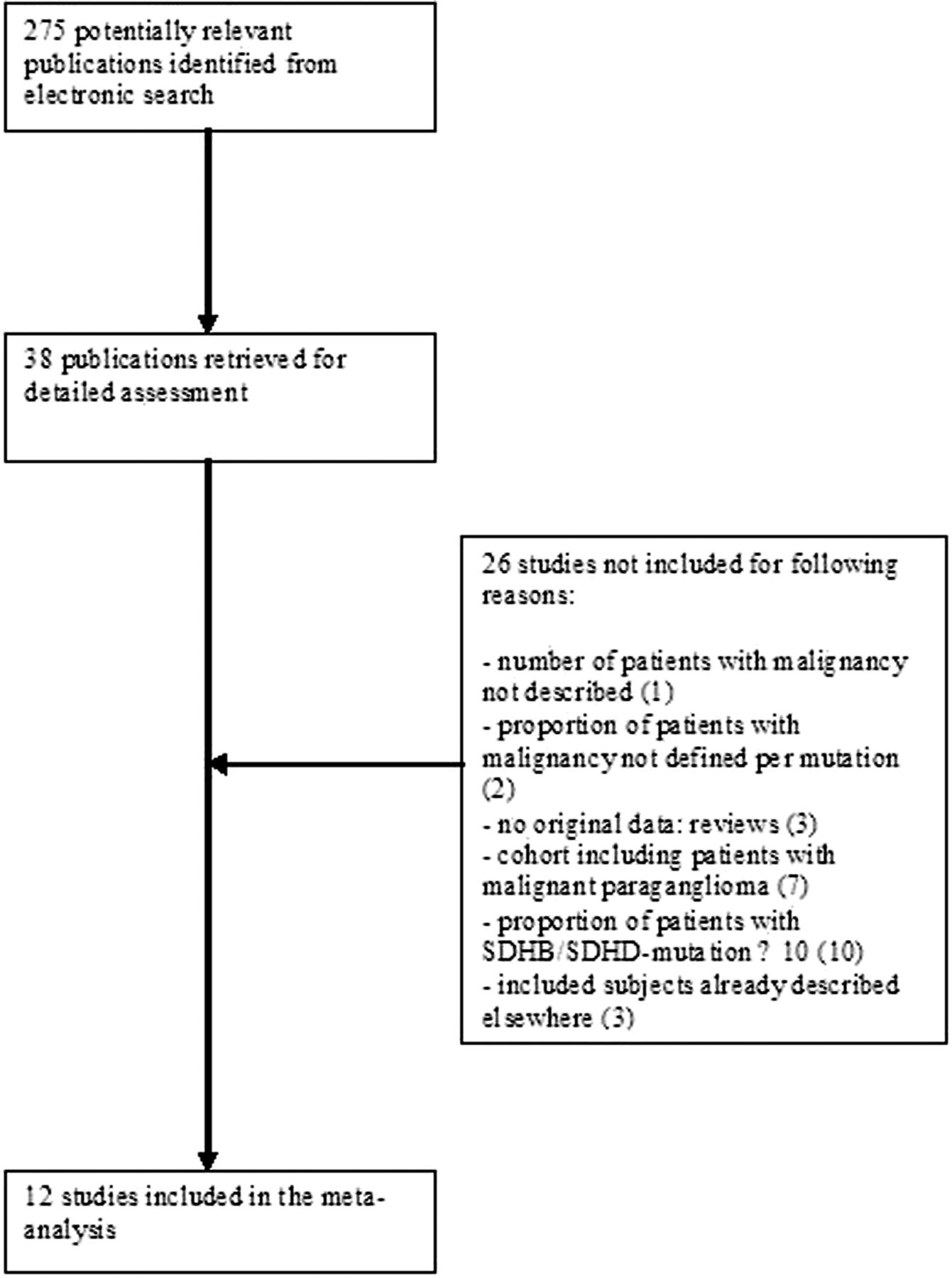
Flow-diagram of study selection.
Ten studies were excluded because the number of subjects with an SDHB-mutation or SDHD-mutation did not exceed 10.34–43 Furthermore, three studies comprised a population, already described in publications included in our review; the studies with the smallest sample sizes were excluded.9 ,18 ,44 No new articles were found in references of key articles. Finally, a total of 12 studies were included in the present analysis, all written in English.12 ,14 ,15 ,17 ,45–52
Risk of bias assessment
Characteristics of the risk of bias assessment are shown in table 1. Determination of exposure (SDHB-mutation or SDHD-mutation) was adequately reported in all studies except one, in which the method of molecular genetic testing for mutations was not described.17
Risk of bias assessment of included studies
An adequate definition of metastatic PGL according to our prespecified definition was used in all articles but one.45 In this study, malignant PGL was defined as the presence of distant metastases or local invasion. Since the presence of distant metastases meets our eligibility criteria for defining malignant PGL, we decided to include this study for our review. However, since we were not able to make a distinction between patients in whom a diagnosis of malignant PGL was based on the presence of distant metastases, and patients in whom it was based on the presence of local invasion, we could not exclude data of these latter ones from our results. This may have led to an overestimation of the risk for malignancy.
Eight studies (67%) used an adequate assessment of metastatic PGL according to our prespecified definition. In the other studies, diagnostic work-up included self-reported clinical information,45 family history reports from close relatives,51 or was not clearly reported.14 ,17
In all but one study51 it was unclear whether exposure was unrelated to the outcome, that is, whether genetic screening was initially performed because of the presence of metastatic disease. This means that the majority of studies do have a high risk of selection bias, with potential overestimation of the risk for malignancy. Actual loss to follow-up in both cohort studies was reported to be more than 10%.14 ,52
Study characteristics
Individual study characteristics are displayed in table 2. Included studies were published from 2003 to 2011. Two studies were classified as cohort studies,14 ,52 10 as cross-sectional studies.12 ,15 ,17 ,45–51 In two manuscripts, solely SDHB-mutation carriers were studied,51 ,52 in three studies, solely SDHD-mutation carriers,45 ,47 ,49 and in seven studies both mutations were studied.12 ,14 ,15 ,17 ,46 ,48 ,50 For SDHB-mutation carriers, the total number of patients analysed for malignant PGL was 506; the largest study comprised 295 carriers.50 For SDHD-mutation carriers, the total number of patients analysed for malignant PGL was 549; with 195 in the largest study.12
Characteristics of included studies (in alphabetical order)
Mean age at first diagnosis of PGL ranged from 28.7 to 47.1 years in SDHB-mutation carriers, and from 26.5 to 39.7 years in SDHD-mutation carriers. The two cohort studies reported follow-up durations of median 48 months and mean 70 months, respectively.14 ,52
Risk of malignant PGL: meta-analysis
Table 3 gives an overview of reported incidences and prevalences of included studies. Benn et al reported an incidence of malignant PGL of 19% in SDHB-mutation carriers, and of 8% in SDHD-mutation carriers after a median 48 months of follow-up.14 Srirangaligam et al report an incidence of malignant PGL in SDHB-mutation carriers of 16% after a mean 70 months of follow-up.52 Reported incidences in these two cohort-studies were not stratified for patients with manifest disease and asymptomatic mutation carriers at time of entering the study.
Reported prevalences and incidences
Prevalences of malignant PGL reported in studies concerning patients with manifest disease ranged from 0% to 54% for SDHB-mutation carriers, and from 0% to 23% for SDHD-mutation carriers. In studies comprising both asymptomatic mutation carriers and patients with manifest disease, the reported prevalence ranged from 3% to 34% for SDHB-mutation carriers, and from 0% to 7% for SDHD-mutation carriers. None of the studies reported incidence or prevalence for asymptomatic mutation carriers only.
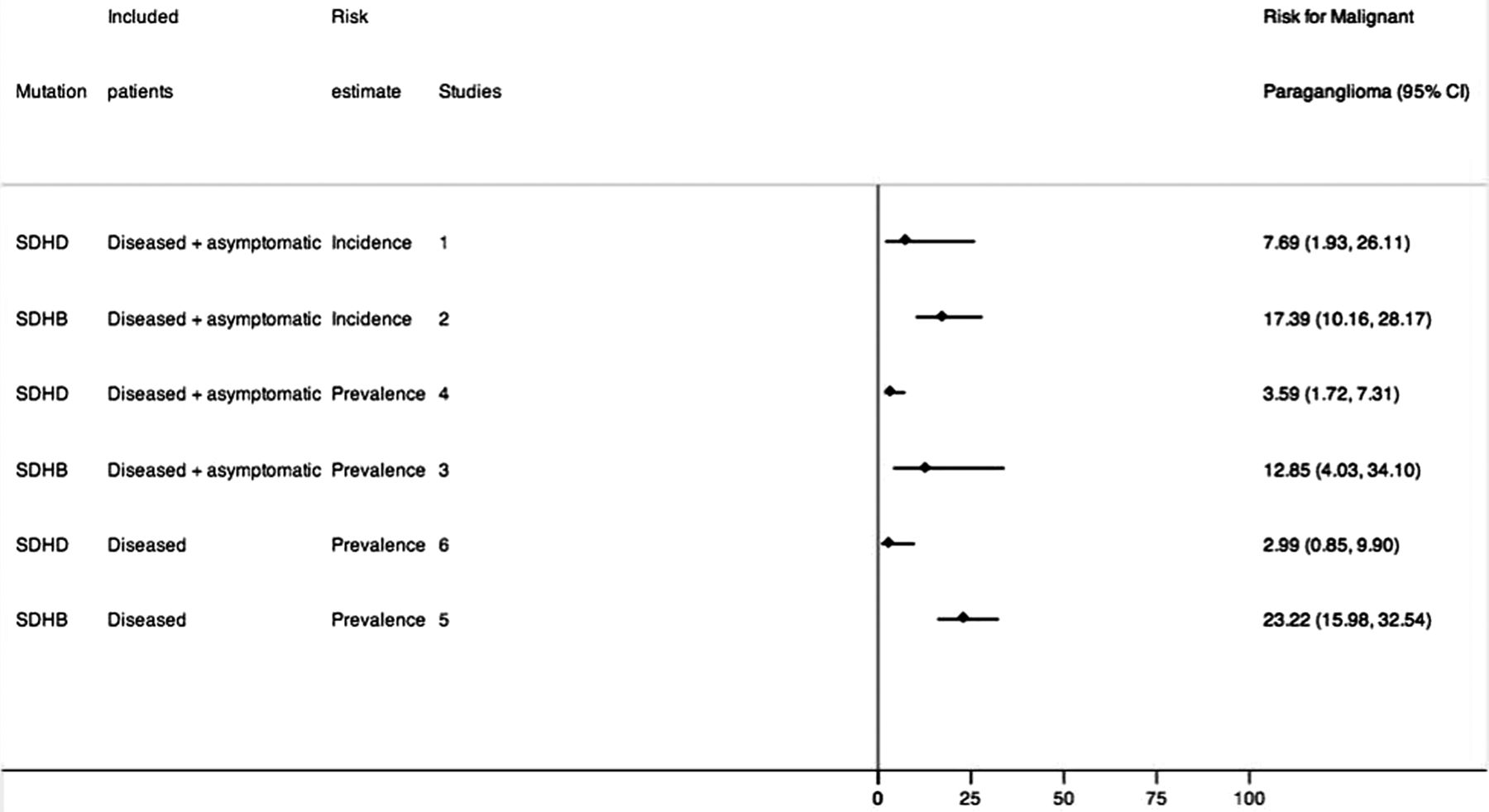
Results of the meta-analysis, stratified for risk estimate, mutation and population are shown in figure 2. All analyses were performed with a random effects model. The pooled risk of malignant PGL in incidence studies comprising both asymptomatic mutation carriers and mutation carriers with manifest disease was 17% (95% CI 10 to 28) for SDHB-mutation carriers, and 8% (95% CI 2 to 26) for SDHD-mutation carriers. The pooled risk in prevalence studies was 13% (95% CI 4 to 34) and 4% (95% CI 2 to 7), respectively. In prevalence studies comprising only mutation carriers with manifest disease, pooled risk was 23% (95% CI 16 to 33) for SDHB-mutation, and 3% (95% CI 1 to 10) for SDHD-mutation carriers. Because of the small number of included studies, a meta-regression to quantify the potential risk of bias was not performed.
{kind=link}
{kind=link}
Meta-analysis.
Discussion
Principal findings
The present systematic review and meta-analysis aimed to assess the risk of developing malignant PGL in SDHB-mutation and SDHD-mutation carriers. Our study showed a pooled incidence of 17% and 8% in SDHB-mutation and SDHD-mutation carriers, respectively. The pooled risk in prevalence studies ranged from 13% to 23% in SDHB-mutation carriers, depending on presence of manifest disease, and 3%–4% in SDHD-mutation carriers. These data show that SDHB-mutations are associated with a higher risk of developing malignant PGL than SDHD-mutations.
High percentages of malignant PGL in SDHB-mutation carriers have already been reported.1 ,11 However, in these studies patients who already suffered from malignant PGL were tested for the presence of SDHB-mutation or SDHD-mutations, which leads to an unreliable prevalence estimation. By excluding studies that sampled patients based on the outcome (ie, malignant PGL), the results from our meta-analysis show that the pooled risk estimation in SDHB-mutation carriers is lower than hitherto appreciated. Therefore, with the results of this study, it is possible to inform SDHB-mutation or SDHD-mutation carriers more adequately concerning their risk of developing malignant PGL.
Limitations
The 12 included studies showed a high risk of bias. First, it was unclear in the majority of studies whether genetic testing was performed because of the presence of metastatic disease. This means that these studies are prone to selection bias, thereby potentially increasing the risk estimates falsely. Since most studies included, for the greater part, patients with manifest disease, of whom a substantial proportion were in tertiary care centres, we assume that most included patients concern index cases with a higher than average risk of harbouring malignant disease. Hence, this referral bias might also overestimate the prevalence of malignant PGL.
Furthermore, as is mentioned in table 2, three studies recruited subjects from the same international registry.15 ,46 ,49 Since this may have resulted in a possible overlap in the included study populations, this may also have contributed to an overestimation of the prevalence of malignant PGL.
We were able to include only two cohort studies, with respective follow-up durations of median 48 months and mean 70 months.14 ,52 The paucity of cohort studies with a long-term follow-up is probably due to the fact that SDH gene mutations have only been described quite recently. However, it is reported that metastatic disease can occur up to 20 years after initial diagnosis of PGL.53 ,54 The lack of long-term follow-up in the two included cohort studies may have resulted in an underestimation of the incidence of malignant PGL.
Three studies examined patients with only one specific mutation; that is, the SDHD D92Y mutation by Hensen et al, the SDHD Cys11X mutation by Peczkowska et al., and the SDHB exon 1 deletion by Solis et al.47 ,49 ,51 It has been shown that as mutations are spread out across the SDHB or SDHD genes, there are no particular hot spots for mutations.55 Inclusion of studies which only focus on one specific mutation may have skewed our results, since it is unknown if these specific mutations are more or less likely to be associated with malignant potential.
Another important limitation is that 33% of the included studies did not adequately assess metastatic PGL, thereby increasing heterogeneity of the included studies. This could have biased the risk estimates, for instance, when in studies, the diagnostic work-up relied also on clinical information reported by family members. We aimed to use elements of risk of bias assessment to explore potential heterogeneity between studies, but due to the small number of included studies, performing a sensitivity analysis was not feasible.
Generalisability of study results
Studies assessing the risk of developing malignant PGL in SDHB-mutation or SDHD-mutation carriers were included in the meta-analysis. However, most studies included patients from international registries, while the frequency of founder mutations and corresponding penetrance may vary in different countries. Furthermore, these registries mostly comprised symptomatic patients treated in tertiary care centres. These selection mechanisms prohibit simple generalisations of the study results.56 The question arises whether malignant PGL has been overdiagnosed on the basis of cross-sectional studies concerning mostly index cases. Therefore, results of the present study are probably only applicable to symptomatic patients seen in referral centres.
Recommendations for future research
This meta-analysis assessed the risk of developing malignant PGL in SDHB-mutation and SDHD-mutation carriers. However, none of the included studies concerned follow-up studies of asymptomatic mutation carriers. To be able to provide newly diagnosed, asymptomatic mutation carriers with accurate information of their risk of developing malignant PGL, prospective follow-up studies in asymptomatic mutation carriers are urgently needed.
Conclusions
In conclusion, the present study shows that the risk of developing malignant PGL is higher in SDHB-mutation than in SDHD-mutation carriers, but lower for SDHB-mutation carriers than hitherto appreciated. However, reported risks on developing malignant PGL in SDHB-mutation or SDHD- mutation carriers vary considerably in the included studies, due to methodological differences, including selection bias. To provide SDHB-mutation and SDHD-mutation carriers with accurate prognostic information concerning their risk of developing malignant PGL, further research is warranted.
Acknowledgments
The authors would like to thank J W Schoones for his help in conducting the literature search.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online appendix
Footnotes
-
Contributors LH performed the literature-search, extracted data for analysis and wrote the article. OD conducted the meta-analysis and wrote the article. FH extracted data for analysis and revised the manuscript. JS revised the manuscript. EC had the idea for the article, extracted data for analysis and revised the manuscript. She is guarantor. All authors read and approved the manuscript.
-
Competing interests None.
-
Provenance and peer review Not commissioned; externally peer reviewed.