Article Text

Abstract
Background: Selection for genetic testing of BRCA1/BRCA2 is an important area of healthcare. Although testing costs for mutational analysis are falling, costs in North America remain in excess of US$3000 (UK price can be £690). Guidelines in most countries use a 10–20% threshold of detecting a mutation in BRCA1/2 combined within a family before mutational analysis is considered. A number of computer-based models have been developed. However, use of these models can be time consuming and difficult. The Manchester scoring system was developed in 2003 to simplify the selection process without losing accuracy.
Methods: In order to increase accuracy of prediction, breast pathology of the index case was incorporated into the Manchester scoring system based on 2156 samples from unrelated non-Jewish patients fully tested for BRCA1/2, and the scores were adapted accordingly.
Results/Discussion: Data from breast pathology allowed adjustment of BRCA1 and combined BRCA1/2 scores alone. There was a lack of pathological homogeneity for BRCA2, therefore specific pathological correlates could not be identified. Upward adjustments in BRCA1 mutation prediction scores were made for grade 3 ductal cancers, oestrogen receptor (ER) and triple-negative tumours. Downward adjustments in the score were made for grade 1 tumours, lobular cancer, ductal carcinoma in situ and ER/HER2 positivity. Application of the updated scoring system led to four and nine more mutations in BRCA1 being identified at the 10% and 20% threshold, respectively. Furthermore, 65 and 58 fewer cases met the 10% and 20% threshold, respectively, for testing. Moreover, the adjusted score significantly improved the trade-off between sensitivity and specificity for BRCA1/2 prediction.
Statistics from Altmetric.com
Mutations in BRCA1 and BRCA2 confer a marked increased lifetime risk of developing breast and ovarian cancers and have a propensity to give rise to cancer at a young age. Consequently, despite contributing to less than 5% of new breast and 15% of new ovarian cancer diagnoses, it has been shown to be beneficial for healthcare systems to screen for these patients before providing surveillance, prevention or therapeutic strategies. The challenge for the clinician is to identify the subset of patients who are most likely to benefit from costly genetic testing. Even at extremes of age, the presence of a BRCA1/2 mutation will confer higher risks.1
A number of models and scoring systems have been derived to assess the probability of a BRCA1 or BRCA2 mutation in a given individual dependent on their family history.2 Some earlier probability models such as those of Couch et al3 and Shattuck-Eidens et al4 were derived before widespread genetic testing had been introduced. Two tabular scoring systems have also been derived from the Myriad Genetics Laboratories testing programme.5 6 However, the most widely used and validated model is BRCAPRO,7 8 which requires computer entry of the family history information. In 2003, we developed the Manchester scoring system to facilitate a simpler and more accurate selection of families for BRCA1/2 testing (table 1).9 This development was undertaken primarily because existing systems were either laborious or had little validation. Since that time, the Manchester scoring system has compared well with existing models such as BRCAPRO and Myriad as well as the newer BOADICEA model.9 10 11 12 13
Manchester scoring system
Recent evidence has shown that the type of breast pathology, including hormonal receptor status, can influence the chance of detecting a BRCA1, but not so much a BRCA2, mutation, and these factors have been incorporated into the BRCAPRO model and are in the process of being incorporated into BOADICEA. Therefore it appears timely to assess incorporation of breast pathology into the Manchester scoring system and to determine what effect this has on the model’s performance as well as its continued ease of use in the clinic setting.
Patients and methods
The Manchester scoring system was initially developed using parameters outlined in table 1. The score was derived from two datasets and validated in a third.9 14 Although initially used to discriminate for each BRCA gene in isolation at the 10% detection threshold, a combined score for mutation prediction for both genes has now also been validated.12 13 14 In our clinics, we use a combined score of 16 points for the 10% threshold and 20 points for the 20% threshold of mutation probability. We have already assessed the effect of pathology in ovarian cancer on the scoring system,15 but now determine the additional effect of the proband’s breast pathology in addition to ovarian pathology. We reviewed the data available to us from hospital records, pathology reports and cancer registries on 1918 breast cancer index cases out of 2156 non-Jewish index cases (238 cases had ovarian cancer only) who were fully tested for BRCA1/2 including multiple ligation-dependent probe amplification, which detects large single-exon or multi-exon deletions and duplications. Oestrogen receptor (ER) status was taken as negative if the quick score was 0/8 or if <5% cells were positive by immunohistochemistry. Her2 was regarded as positive if the tumour showed gene amplification by fluorescent in situ hybridisation (FISH) or, in the absence of FISH, if the immunohistochemical “Hercept test” was 3+ (scale of 0–3) Adjustments were made to the Manchester Score of the index case based on the following variables: tumour grade, lobular pathology, ductal carcinoma in situ (DCIS), ER and Her2 receptor status. In addition, a detailed pathology and receptor review was carried out in 113 breast cancer cases from a population-based study of women diagnosed aged <31 years.16 In all other instances, only available pathology data from cancer registries and hospital records were used. Multiple analyses using additions or subtractions were performed until the best discriminating set was identified. Modifications to the Manchester Score were made for variables that differed substantially between the BRCA1 and BRCA2 datasets and the non-BRCA1/2 datasets, particularly samples testing negative for both BRCA1 and BRCA2. The accuracy of the adjusted scoring system was assessed by the overall sensitivity and specificity of the model, as well as its positive and negative predictive value. In addition to the accuracy, the discriminatory precision for individual cases was evaluated using receiver operating characteristic (ROC) curves. These are plots of the true positive rate against the false positive rate for different possible cut-off points and hence show the trade-off between sensitivity and specificity. For binary outcomes, the concordance statistic (C-statistic) is equivalent to the area under the ROC curve. Therefore, the Wilcoxon estimate of the area under the ROC curve was calculated for the original and adjusted models.
Results
Although breast cancer was confirmed in all cases, the reporting system for pathology in the UK meant that reliable data on tumour grade were not available for most cases until 1990 and for ER until 1996. Furthermore, Her2 was only widely reported after 2001. Consequently, as a large number of index cases were diagnosed with breast cancer between 1960 and 1990, pathology data (which included at least grade of tumour) were obtained on 1116 cases (57%) only (table 2). ER status was available for 707 (37%) of these patients and Her2 for 286 (15%). BRCA1 tumour pathology data were available in 126/203 (62%) breast cancer index cases, and ER status was available in 43%. Table 2 shows the distribution of pathological subtypes in the sporadic, familial and BRCA1/2 patients. As expected, BRCA1 tumours were typically grade 3 invasive ductal cancers, which, where results were available, were mainly ER and Her2 receptor negative. Fifty-one of 87 BRCA1 cancers (63%) fulfilled the “triple-negative” criterion. BRCA1 cancers were 4–5-fold less likely than non-BRCA1 tumours to be lobular or grade 1. No BRCA1 tumours overexpressed Her2. In contrast, the pathological heterogeneity between BRCA1 and non-BRCA1/2 cases was not demonstrated with BRCA2. No striking differences were seen in the distribution of histology and receptor status in tumours from BRCA2 and non-BRCA1/2 familial breast cancer patients.
Available breast pathology and receptor status in 1116 index cases tested for BRCA1 and BRCA2 mutations
Consequently, the Manchester scoring system was modified for BRCA1 probability alone. Adjustments of 0–4 points (upwards or downwards) were considered for all histological and receptor variables. Features that were less prevalent in BRCA1-associated tumours were given a negative score, and those more prevalent in BRCA1 tumours were given a positive score. Scores above 4 were not investigated because our data showed that, even for a triple-negative breast cancer patient under 31 years of age with no family history, the frequency of constitutional BRCA1 mutation was 2/16 (12.5%) and therefore only just reached the 10% likelihood for BRCA1. In other words 4 additional points added to the usual 6 for a breast cancer patient <30 years of age (table 1) adds up to 10 points, the BRCA1 10% threshold. Of interest, the frequency of BRCA1 mutations found in a similar woman with sporadic, pathological grade 3 and ER-negative (rather than triple-negative) breast cancer was just 9% (2/22). In such cases, the 6 points attained for a breast cancer in a patient in their 20s plus 4 points for a triple-negative tumour would also just reach the 10 point 10% threshold for BRCA1, whereas, if it were only pathological grade 3 and ER negative, it would score 9 points and not reach the testing threshold. The maximum for downward adjustment was based on the premise that, even if a woman at 50% risk of a known BRCA1 mutation developed an atypical tumour for BRCA1, she would still have at least a 50% risk of a family mutation. As such, a score of 20 points (equivalent to a 20% risk) should not be reduced below 16 points (equivalent to a 10% risk of either BRCA1 or BRCA2).
After the pathology score had been considered, multiple analyses were carried out to determine adjustments that best discriminated between the probability or not of BRCA1 mutations in an individual. Table 3 shows the adjustments based on breast pathological correlates.
Calculated adjustments to the Manchester Score for predicting BRCA1 and BRCA2 mutations according to pathology and receptor status of breast cancer in the index case and the presence of ovarian cancer in the family
Examples
Grade 3 ER positive would score +1 (+2 for grade 3, and −1 for ER positive)
Grade 3 ER negative would score +3 (+2, +1) unless triple negative (+4) when 4 points added to total score
Grade 1 ER positive scores −3 (−2, −1), 3 points deducted from total score
Grade 2 but no receptor status known (0), no adjustment
Lobular carcinoma ER positive would score −3 (−2, −1)
Adjusting the scores to provide the best adjustments for sensitivity and specificity improved the overall discrimination. For example, at the 10 point BRCA1 total score, 23 BRCA1 mutations were missed with the unadjusted score but only 11 with the adjusted score, and 15 fewer cases required genetic testing. With the use of the combined scoring thresholds of 16 points and 20 points for the 10% and 20% mutation probability thresholds, 65 and 58 fewer samples, respectively, qualified for testing, yet four and 10 more BRCA1 mutations, respectively, were identified (table 4), with the non-identification of only one BRCA2 mutation carrier.
Potential gains from the need to test fewer samples and the detection of more mutations using the adjusted pathology score
Table 5 shows the overall adjustments to scores produced for BRCA1, BRCA2 and non-BRCA1/2 breast cancers. It confirms how index BRCA1/2 cases were more likely to have upward adjustment, whereas index BRCA1/2 negative cases were more likely to have a downward adjustment.
Adjustments performed in the scores of index cases using the Manchester scoring system including pathology and receptor status
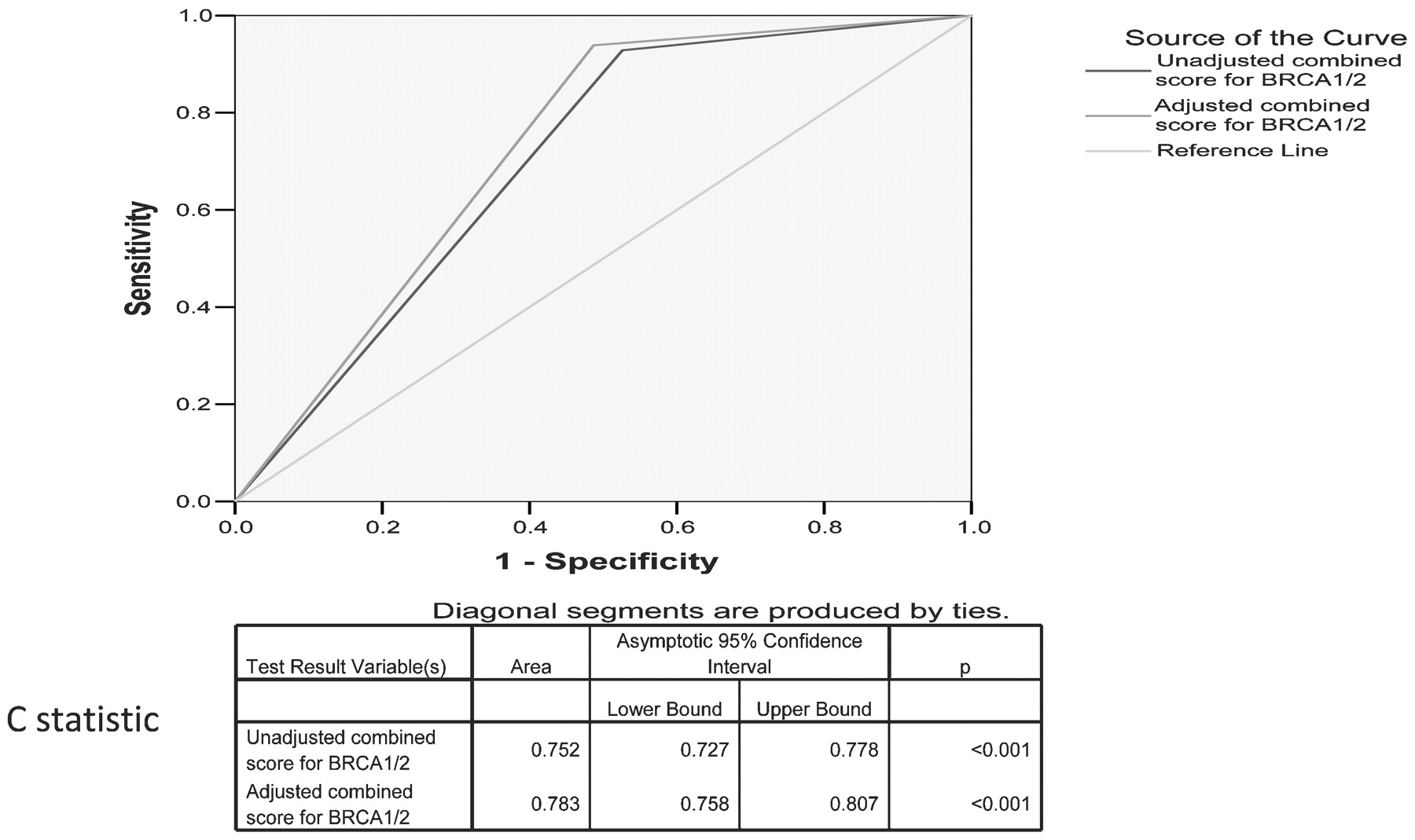
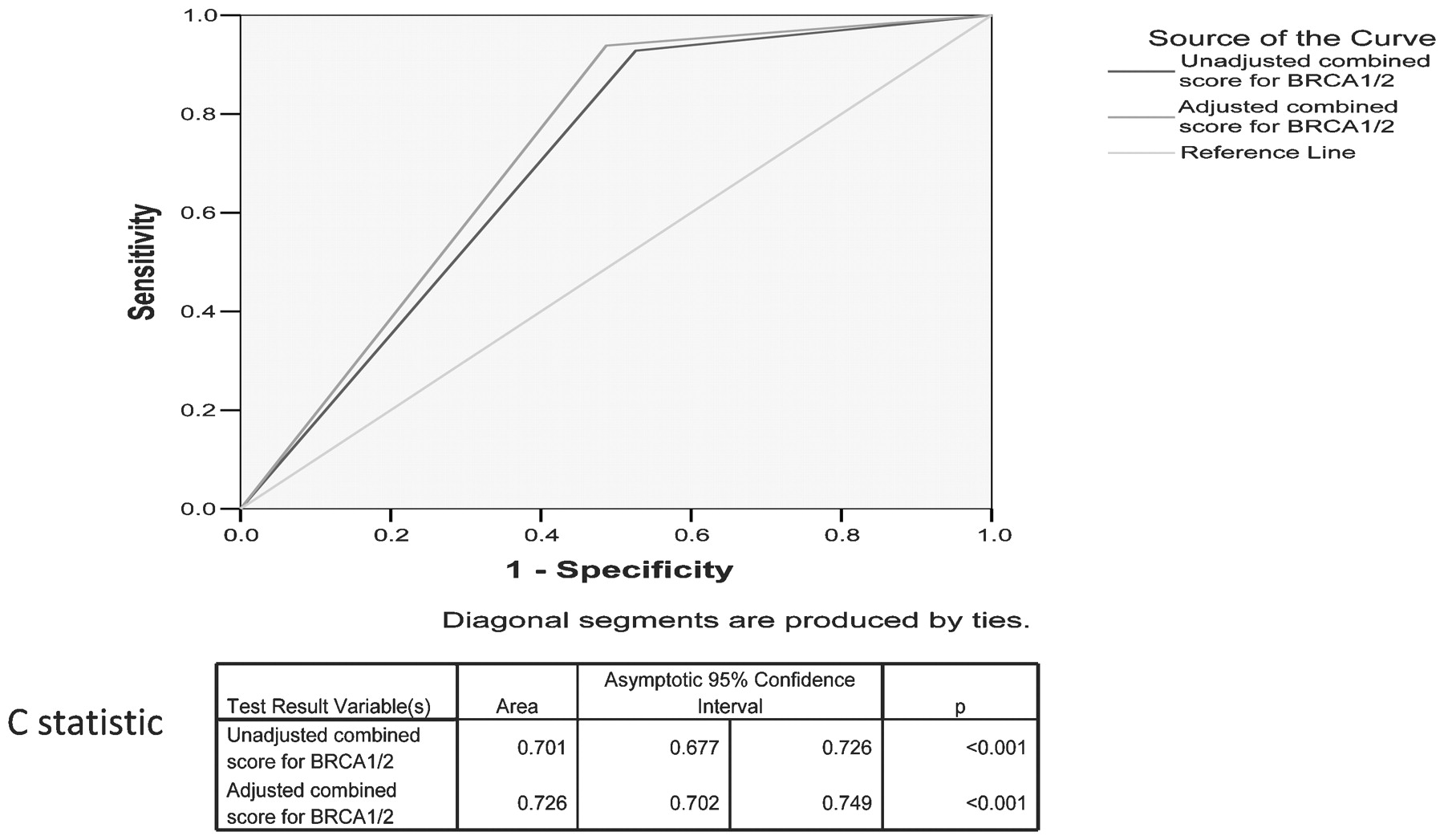
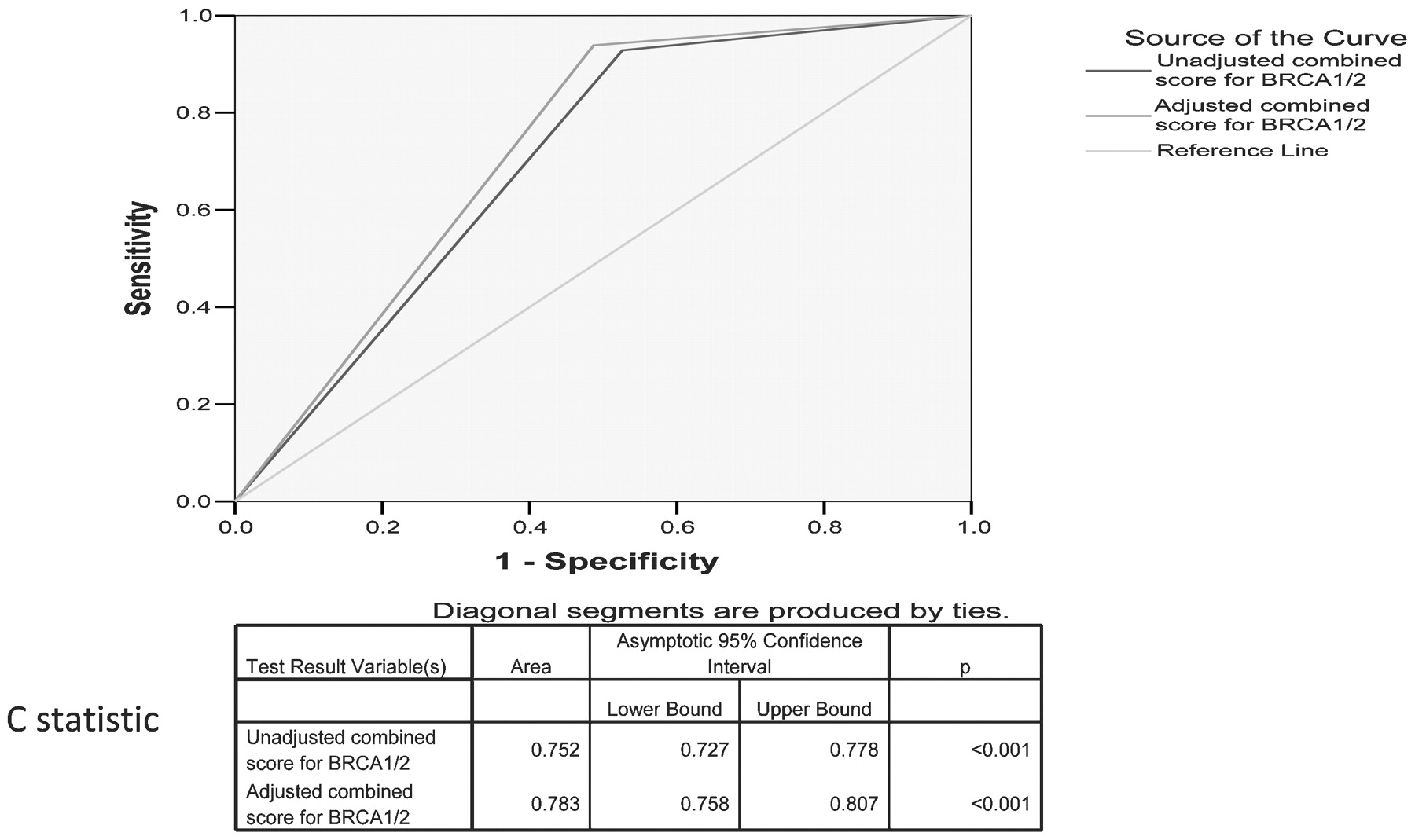
Table 6 shows the sensitivity, specificity, positive predictive value and negative predictive value for the unadjusted and adjusted model. Figures 1 and 2 show the ROC curve estimates for BRCA1 and combined BRCA1/2 scores and C-statistic and 95% CI for these curves at the 10% threshold, respectively. Figure 3 shows the ROC curves for the unadjusted and adjusted Manchester scoring system estimates for the combined BRCA1/2 score at the 20% threshold as well as the C-statistic and 95% CIs for these curves. Overall, these results show that the adjustments we used significantly improved the discriminatory accuracy of the scoring system for both BRCA1 alone (at the 10% threshold) and for the combined BRCA1/2 score at both the 10% and 20% thresholds. This overall improvement was evident despite specific breast pathology data being available for only 43% of cases tested.

Receiver operating characteristic curves for BRCA1 at the 10% threshold.
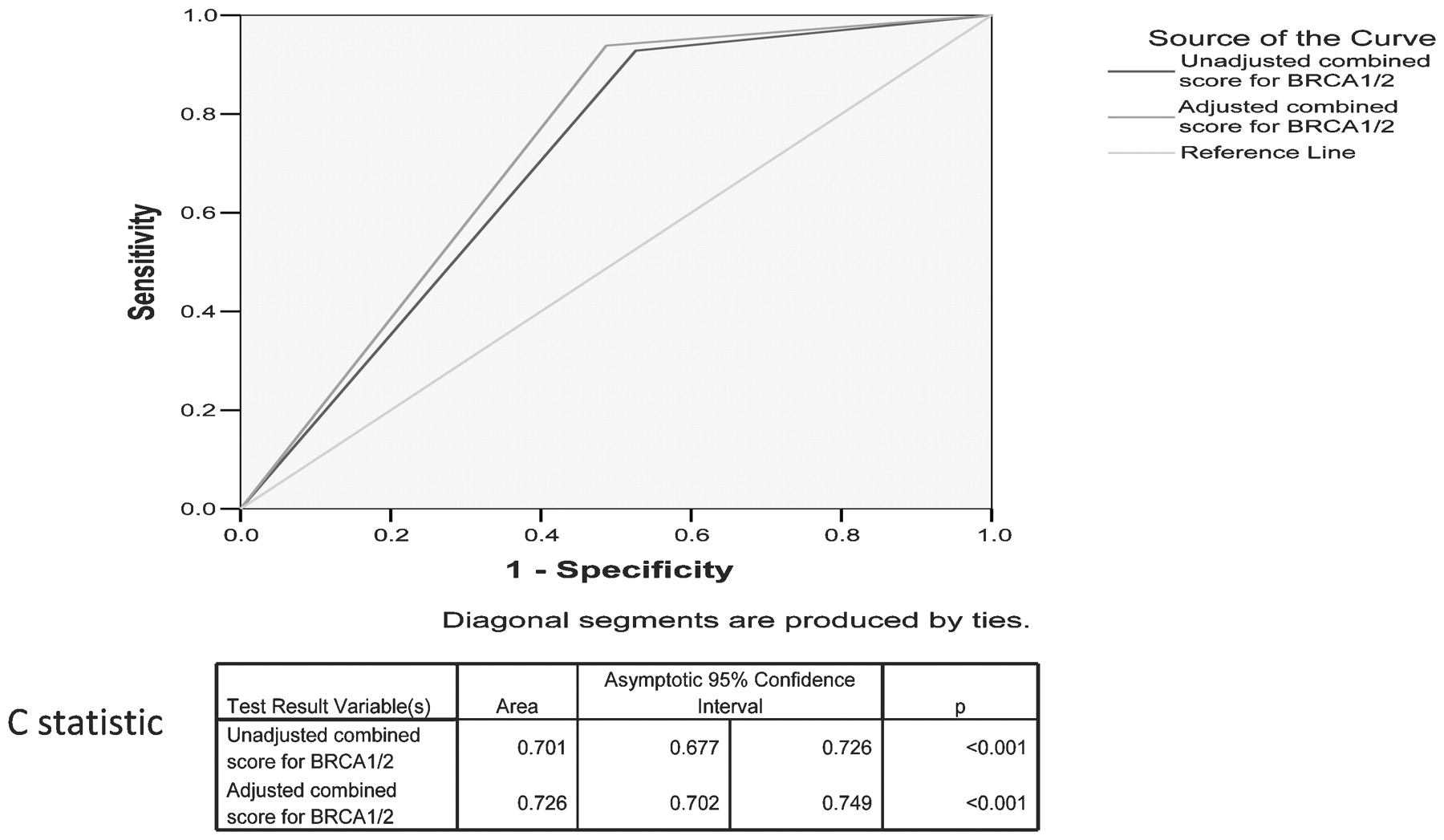
Receiver operating characteristic curves for combined BRCA1/2 using the 10% threshold.
{kind=link}
{kind=link}
{kind=link}
Receiver operating characteristic curves for combined BRCA1/2 using the 20% threshold.
Sensitivity, specificity and positive predictive value of Manchester Scores at 10% and 20% threshold adjusted and not adjusted for pathology and receptor status
We estimate that incorporation of the breast pathology adjustment adds no more than 20 s to the time to calculate the Manchester Score.
Discussion
Accurate, individualised assessment for the risk of BRCA1 or BRCA2 gene mutation is essential to provide clinicians with information on which patients to select for expensive genetic testing. A number of models have been developed to aid clinicians in this process, but many of these are time consuming and hence are difficult to use in busy clinical practices. Our group developed and validated the Manchester Score9 as a quick scoring system to predict BRCA mutation carriers. The model has compared well with existing, as well as newer, models.10 11 12 13 More recently, many of these models, which usually derive their risk from age and family history alone, have been improved by including pathological features of the proband’s breast or ovarian cancer. In this article, we report the result of a validation of the Manchester scoring system adjustment for pathological correlates.
We undertook a pragmatic study using available data from pathology reports and hospital records of women with breast cancer who had BRCA1/2 testing. Available breast pathology data on 1116 breast cancers from patients tested for BRCA1 and BRCA2 were used to develop a modification to the Manchester Score. It was only possible to derive a modification for BRCA1, as BRCA2 tumours were not sufficiently different from sporadic or familial non-BRCA1/2 tumours. Upward modifications of between 1 and 4 points were made for a number of pathological features, including ER negativity (+1), pathological grade 3 (+2) and grade 3 triple negativity (+4). Downward modifications of −1 to −4 were made for ER positivity (−1), DCIS (−1), pathological grade 1 (−2), lobular cancer (−2), lobular carcinoma in situ (−3) and Her2 positivity (−4). These results, based on a large series of familial breast cancer cases, show that pathology in the proband can be used effectively to significantly improve the discrimination of the Manchester scoring system. This improvement was seen not only in overall accuracy, as evidenced by improved sensitivity and specificity, but also for individualised risk assessment, as evidenced by significant improvement in concordance statistics derived from ROC curves.
As has been shown in previous studies,17 18 19 20 our data have confirmed that BRCA1-related breast cancers were more likely to be pathological grade 3 invasive ductal cancers and to be ER and Her2 negative. Tumours were also less likely to be pathological grade 1 or lobular. The need to discriminate is greatest for familial rather than sporadic breast cancers. Nonetheless, the question remains as to which sporadic patients should be offered formal BRCA gene testing. Population-based studies of early-onset breast cancer in outbred non-founder populations have reported a low (<10%) rate of BRCA1/2 mutations in diagnosed women with no family history.16 21 22 Lakhani et al17 have provided data on the likelihood of breast cancer being caused by a BRCA1 mutation by pathological grade and ER status at various ages. These data were for all women, not those without a family history. Women aged 20–29 years with grade 3 ER-negative breast cancers had a 35% chance of a BRCA1 mutation, with a similarly high risk (26.5%) for women aged 30–34 years. Only after the age of 34 years did the risk fall below 10%.17 Unfortunately, it appears that some clinicians have misinterpreted these data and called for all women under 35 years of age with pathological grade 3 and ER-negative breast cancer to be tested or offered testing based on a 10–20% testing threshold. The population-based data presented in this article confirm a similar 29% risk for young women (age <31years). However, these data were derived from all women, not those without a family history. For sporadic breast cancer, the mutation rate was only 9%, although this rose to 12.5% for triple-negative breast cancer. This suggests that only triple-negative, pathological grade 3 breast cancers in women <31 years qualify for testing irrespective of family history based on guidelines using a 10% threshold in outbred populations. Clearly, the confidence intervals are wide on these numbers, and further studies to assess the rates of mutations in sporadic triple-negative patients will help inform models and scoring systems further. Thresholds may also change if BRCA1/2 status becomes more important in determining choice of treatment regimen, such as with the validation of use of poly(ADP ribose) polymerase inhibitors. These have been shown to have preferential activity in BRCA-mutated women.23 24 When such treatment becomes validated, testing thresholds will need to be reassessed.
The methodology used in this article may be criticised for the incompleteness of pathological data and for its retrospective analysis. However, this largely pragmatic approach, although a potential failing of the analysis, is similar to the approach that clinicians are faced with when deciding to test a family in the clinic. Although UK guidelines for testing use a 20% threshold,25 these are not universal. However, they are especially important in nationally funded healthcare systems. Even outside these systems, insurance companies are likely to insist on some sort of a threshold before funding a test. Pathology characteristics are now being incorporated with some success into computer models such as BRCAPRO26 and BOADICEA.27 Adjustments in the total score can be made to account for lower breast cancer incidence such as a 15 point, 10% threshold score in Malaysia, where the Manchester Score was as effective or better than BOADICEA.28 The Manchester Score has been independently validated as taking 40 s per family tree.29 We estimate that addition of the pathology will add no more than 20 s to the time required. Clinicians and genetic counsellors wishing to use the simpler Manchester scoring system can now improve the prediction in families by incorporating a pathology score for the breast cancer in the index case at the cost of minimal extra time.
Conclusion
The adjusted Manchester scoring system enables a more accurate prediction to be made of the likelihood of a given individual having a mutation in BRCA1 or BRCA2. We would suggest using the basic scoring system and then adjusting scores using pathology information to enable accurate prediction and best use of limited financial resources.
Acknowledgments
We acknowledge the tireless support of Andrew Shenton who carried out much of the statistical analysis but died tragically young before submission. We also acknowledge the support of the Biomedical Research Centre at Central Manchester Foundation Trust.
REFERENCES
Footnotes
Competing interests None.
Ethics approval Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.