Article Text

Abstract
We report the association of CDH1/E-cadherin mutations with cleft lip, with or without cleft palate (CLP), in two families with hereditary diffuse gastric cancer (HDGC). In each family, the CDH1 mutation was a splicing mutation generating aberrant transcripts with an in-frame deletion, removing the extracellular cadherin repeat domains involved in cell-cell adhesion. Such transcripts might encode mutant proteins with trans-dominant negative effects. We found that CDH1 is highly expressed at 4 and 5 weeks in the frontonasal prominence, and at 6 weeks in the lateral and medial nasal prominences of human embryos, and is therefore expressed during the critical stages of lip and palate development. These findings suggest that alteration of the E-cadherin pathway can contribute to human clefting.
- CL, cleft lip
- CLP, cleft lip with or without cleft palate
- COGENE, Craniofacial and Oral Gene Expression Network Consortium
- HDGC, hereditary diffuse gastric cancer
- NMD, nonsense mediated decay
- CDH1/E-cadherin
- cleft lip/palate
- gastric cancer
Statistics from Altmetric.com
- CL, cleft lip
- CLP, cleft lip with or without cleft palate
- COGENE, Craniofacial and Oral Gene Expression Network Consortium
- HDGC, hereditary diffuse gastric cancer
- NMD, nonsense mediated decay
Cleft lip, with or without cleft palate (CLP), occurs in 0.4–2.0 of every 1000 births and represents the most common craniofacial birth abnormality. Most CLP are non-syndromic and familial aggregation and recurrence risks among siblings clearly indicate the involvement of genetic factors.1 Identification of the genes involved in Mendelian syndromic CLP would allow the recognition of pathways which are altered in human clefting and variants of such major genes may correspond to genetic risk factors for non-syndromic CLP.2
METHODS
We identified a family whose clinical presentation strongly suggests that CDH1/E-cadherin mutations may result in CLP. In this family of Caucasian origin, the index case (III-3, fig 1A) died from peritoneal carcinosis at age 23. The proband’s father (II-4) had developed diffuse gastric cancer at the age of 48, and the paternal grandfather (I-1) had died at 36 years of age from gastric cancer. Remarkably, the index case and three relatives who were unaffected at the time, his brother (III-4), his paternal uncle (II-2), and his paternal cousin (III-1), had CLP (fig 1A). The paternal cousin then presented at 22 years of age with epigastric pains. Systematic endoscopy and multiple biopsies of the gastric mucosa revealed the presence of tumour cells. This led to gastrectomy which confirmed the diagnosis of diffuse gastric cancer. Sequence analysis of CDH1 from peripheral blood genomic DNA of the index case (fig 1B) identified a mutation of the intron 4 splicing donor site (c.531+2 T→A; GenBank RefSeq file accession number NM_004360). RT-PCR analysis of CDH1 from peripheral blood lymphocytes and sequence analysis of the amplified cDNA demonstrated that this mutation induced complex aberrant splicing (fig 1C), that is, (i) a complete retention of intron 4 (125 bp), resulting in a premature stop codon within intron 4 at nt 97, and (ii) an in-frame 63 bp deletion of exon 4 (c469_531del), resulting from the activation of an exonic cryptic donor splicing site (nt 469). The CDH1 mutation was present in the proband’s affected cousin (III-1) and asymptomatic paternal uncle (II-2). Subsequently, the proband’s uncle (II-2) underwent a gastrectomy which revealed diffuse gastric cancer with metastatic nodes. In the asymptomatic proband’s 20 year old brother (III-4), gastroscopy as well as biopsies were normal. However, he underwent presymptomatic testing which indicated that he was also a carrier. Since it has been shown that, in hereditary diffuse gastric cancer (HDGC), normal endoscopy and biopsies do not exclude the presence of malignant cells in CDH1 mutation carriers,3 the proband’s brother underwent prophylactic gastrectomy which revealed approximately 80 microscopic foci of intramucosal signet ring cell adenocarcinoma. Therefore, the index case, his paternal cousin, his paternal uncle, and his brother, all presenting with a CLP, carried the CDH1 mutation (fig 1A).

Cosegregation of CLP with CDH1 mutation in an HDGC family. (A) Partial pedigree of family. (B) Detection of the c.531+2 T→A mutation by sequence analysis. Absence of the mutation in the index case’s aunt revealed that the breast cancer was a phenocopy. (C) Schematic representation of the aberrant transcripts detected in blood of relative III-4 presenting an HDGC and a CLP.
The involvement of germline CDH1 mutations in the genetic determinism of CLP was subsequently supported by another family with HDGC (fig 2A). The proband of Caucasian origin (II-3) underwent a gastrectomy for diffuse gastric cancer at 28 years of age. A sister (II-2) had died at age 18 from metastatic diffuse gastric cancer and the father (I-1) had developed gastric cancer when he was 37 years old. The family was then referred to a medical geneticist and participated in a genetic counselling and screening program. Among the six sibs, subject II-4 had a cleft lip and subject II-6 was diagnosed with congenital scalp aplasia cutis and partial acrania. Screening of the CDH1 gene from peripheral blood genomic DNA of the proband revealed the presence of a splicing mutation (fig 2B) affecting the last nucleotide of exon 8 (c.1137G→A). This mutation was present in the affected father (I-1) and also in relatives II-4 and II-6. RT-PCR from blood of relative II-4, presenting with the cleft lip, showed that this mutation resulted, as in the first family, in complex aberrant splicing (fig 2C). One of these aberrant transcripts harboured an in-frame 129 bp deletion corresponding to exon 8 (c1009_1137del).
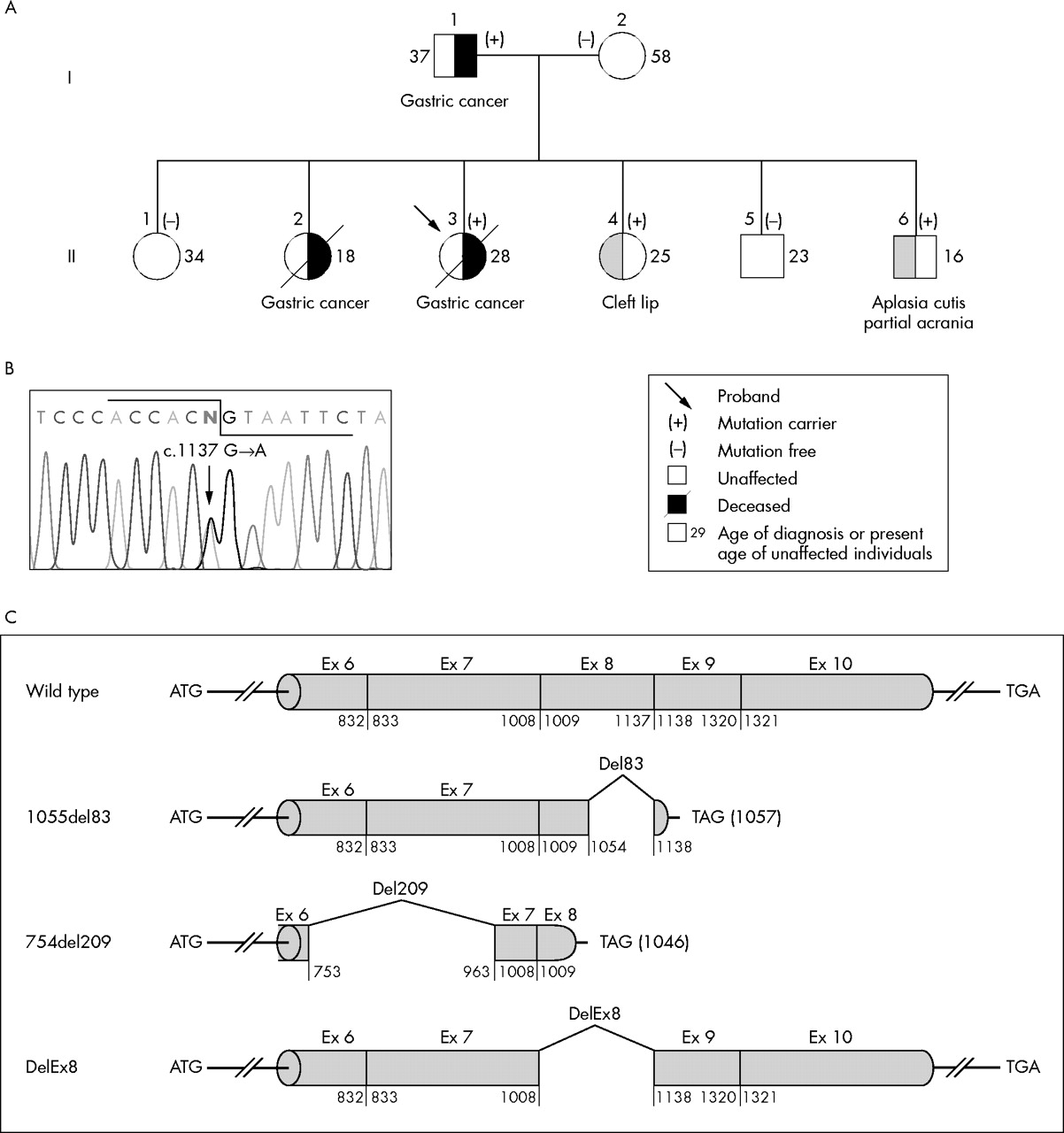
CDH1 mutation in another family with HDGC cancer and CL. (A) Partial pedigree of family. (B) Detection of the c.1137G→A mutation by sequence analysis. (C) Schematic representation of the aberrant transcripts detected in blood of the relative II-4 presenting a CL.
We then investigated the expression profile of CDH1 in oral structures from human embryos. We used the transcriptome data obtained by the Craniofacial and Oral Gene Expression Network Consortium (COGENE), using human Affymetrix microarray hybridisation.4 We found that CDH1 is highly expressed at 4 and 5 weeks in the frontonasal prominence, and at 6 weeks in the lateral and medial nasal prominences (fig 3), and is therefore expressed during the critical stages of lip and palate development. These results are in agreement with previous data obtained in mouse embryos by immunohistochemistry.5 Interestingly, at least at most time points, CDH1 expression covaries with expression of PVRL1, a gene involved in human clefting. Indeed, mutations of the PVRL1 gene, encoding the cell adhesion molecule Nectin-1, cause autosomal recessive syndromic CLP with ectodermal dysplasia (CLPE1 (MIM 225000)6).

{kind=link}
{kind=link}
{kind=link}
COGENE expression profile of CDH1. This profile was compiled from duplicate hybridisations to the Affymetrix U95A chip set and shows the CDH1 and PVRL1 (a known clefting gene) probe set results. RNA samples were derived by micro-dissection of 24 human embryologic structures (listed along the x axis). The y axis represents the differential expression of CDH1 or PVRL1, compared to the median overall intensity. The expression peaks, highlighted with arrows, point out the structures most relevant for lip and palate development, at 4 and 5 weeks in the frontonasal prominence, and at 6 weeks in the lateral and medial nasal prominences.
DISCUSSION
CDH1 mutations, identified in HDGC kindreds, include nonsense, missense, and splice site mutations, and small insertions and deletions,7,8,9,10,11 and these mutations are predicted to result in a loss of function.10 Development of diffuse gastric cancer in CDH1 mutation carriers requires the somatic inactivation of the wild type allele,12,13 as predicted by the Knudson two-hit model, and the tumours show abnormal or absence of E-cadherin expression. Association of CDH1 mutation with CLP has not been reported so far, suggesting that the mutations identified in our two kindreds have a specific effect. In both families, the splicing mutation generated an aberrant transcript with an in-frame deletion which is predicted to escape from the nonsense mediated decay (NMD) pathway.14 The predicted mutant proteins (p.Val157_Gln177del and pSer337-Thr379del, respectively) are probably non-functional, since these 21 and 43 amino acid deletions affect the extracellular cadherin repeat domains (amino acids 36–254, 158–367, and 266–483), required for cell-cell adhesion. Since E-cadherin form dimers,15 such mutant proteins might have potent trans-dominant negative activity over the wild type protein, and this could explain why certain heterozygous CDH1 mutations, escaping from the NMD pathway, may have a phenotypic expression during embryogenesis.
Cell adhesion molecules, such as E-cadherin, are considered to play a major role in craniofacial morphogenesis.2 The cell adhesion molecule Nectin-1, encoded by the PVRL1 gene, mutations in which cause syndromic CLP,6 interacts with E-cadherin. Both proteins are involved in the formation of adherens junctions, which are key structures for cell-cell adhesion.16 Our report suggests that alteration of the E-cadherin pathway can contribute to human clefting.
REFERENCES
Footnotes
-
This work was supported by l’Association pour la Recherche sur le Cancer, La Ligue Nationale Contre le Cancer, and in part by grants from the National Institute of Health (N01 DE92630 to EWJ).
-
Competing interests: none declared