Article Text

Abstract
Methods and results Germline SUFU mutations were identified in two families with several children under 3 years of age diagnosed with medulloblastoma. All medulloblastomas in which the histology was reviewed were of the desmoplastic subtype, including three with the rare extensive nodularity subtype. In both families, the mutation detected in the SUFU gene was a frameshift mutation. Among the 25 mutation carriers identified in the two families, seven developed medulloblastomas.
Conclusions This report highlights three features of SUFU related tumours. These are mainly medulloblastomas with extensive nodularity or typical desmoplastic/nodular medulloblastomas. These tumours mostly, if not exclusively, appear during the first 3 years of life. The penetrance of the mutation is incomplete.
- medulloblastoma
- desmoplastic medulloblastoma
- familial medulloblastoma
- SUFU
- childhood
- genetics
- neuro oncology
- Cancer: CNS
- paediatric oncology
Statistics from Altmetric.com
- medulloblastoma
- desmoplastic medulloblastoma
- familial medulloblastoma
- SUFU
- childhood
- genetics
- neuro oncology
- Cancer: CNS
- paediatric oncology
Medulloblastoma is the most common pediatric brain tumour. Five histologic subtypes are described including classic medulloblastoma, desmoplastic/nodular medulloblastoma, medulloblastoma with extensive nodularity (MBEN), anaplastic and large cell medulloblastoma.1 2 The desmoplastic/nodular subtype is characterised by a double peak of age of onset (one in early childhood, and a second in adolescence and adulthood), location of the tumour in the cerebellar hemispheres, a biphasic tissue pattern, and a favourable outcome. MBEN represents a rare variant described only in young children and is considered as the end of the spectrum of differentiation of desmoplastic/nodular medulloblastoma.3 Involvement of the sonic hedgehog signalling pathway in the genesis of these tumours has been well established with the presence of somatic mutations in Patched 1 (PTCH1),4 suppressor of fused (SUFU)5 or smoothened (SMO)6 mainly in the desmoplastic/nodular subtype.
Most medulloblastomas are sporadic.7 8 However, some genetic syndromes such as the nevoid basal cell carcinoma syndrome (NBCCS) and familial adenomatous polyposis are associated with increased susceptibility to medulloblastoma.9 Several cases of patients with desmoplastic medulloblastoma carrying somatic and/or germline mutations of the SUFU gene have been described.5 10 We now report germline SUFU mutations in two families with several cases of medulloblastoma.
Subjects and methods
Medical histories were obtained by direct interview. All five medulloblastoma specimens for which slides were available were reviewed and classified according to the World Health Organization classification. Written informed consent was obtained for genetic analysis. Blood was collected from the probands and all family members wishing to participate. The 12 exons of SUFU were analysed by direct sequencing (amplification primers are available on request).
Results
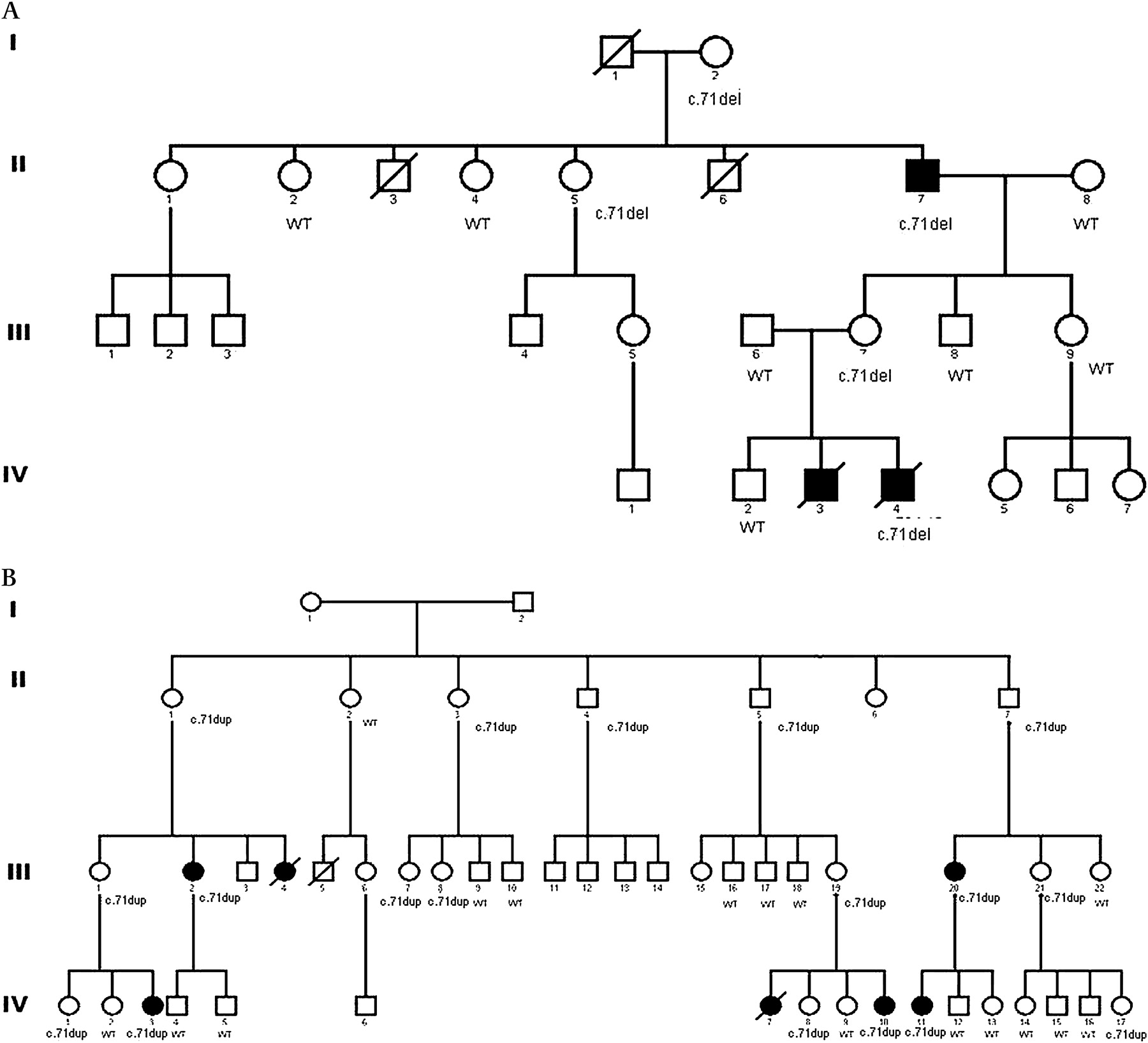
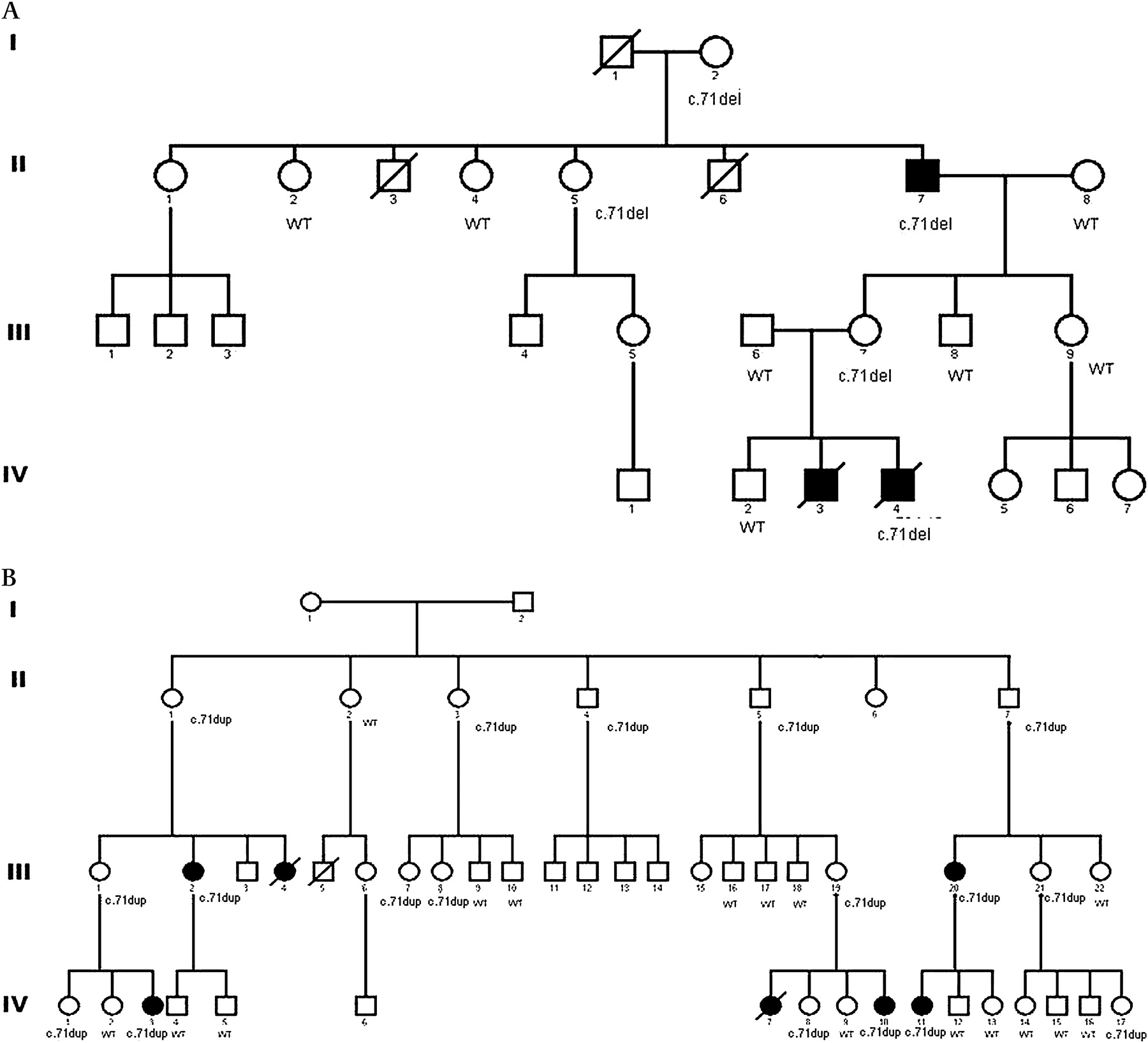
In kindred 1, two sibs were diagnosed with medulloblastoma within the first 3 months of life. None had any associated developmental abnormality. Analysis of the proband's genomic DNA lymphocytes revealed a 1 bp deletion at codon 24 in exon 1 of the SUFU gene (c.71del) leading to a frameshift and a premature stop codon. This mutation was also found in the healthy mother, and in three other family members (figure 1A).
{kind=link}
(A) Kindred 1. All pedigree members for whom DNA was available for genotyping are indicated by either wild type (WT) for SUFU or by c.71del for the mutation carriers. Individuals affected by a tumour are indicated by a filled symbol. The lines through the symbols indicate that the person is deceased. (B) Kindred 2. All pedigree members for whom DNA was available for genotyping are indicated by either wild type (WT) for SUFU or by c.71dup for the mutation carriers. Individuals affected by a tumour are indicated by a filled symbol.
In kindred 2 (figure1B), four patients were diagnosed with a medulloblastoma before 3 years of age. Another child died suddenly at 18 months. Postmortem radiologic findings were consistent with a medulloblastoma. None of these children had any developmental abnormality. Apart from a case of breast cancer and a case of meningioma in late 30s, there was no other tumour case in the family. Seven members of this family died before the age of 3 years, before the era of modern medicine. The sequence of SUFU in the proband's lymphocytes DNA revealed a one bp insertion within codon 24 leading to a frameshift and a premature stop codon (c.71dup). This mutation was also detected in the two children diagnosed with medulloblastoma for whom genomic DNA was available and in 17/33 family members.
No obvious physical stigmata of nevoid basal cell carcinoma syndrome was found among the 21 mutations carriers from both families who have been examined in our clinic, including 11 patients who underwent brain magnetic resonance imaging (MRI).
Relevant data about the tumour cases are summarised in table 1. Medulloblastoma was classified as MBEN in three cases and as typical desmoplastic/nodular medulloblastoma in the other two cases for whom slides were available. In the two medulloblastomas that could be further investigated, one from each family, SUFU sequence analysis documented that only the mutant allele was detected in the tumour DNA, therefore demonstrating the loss of the wild type allele in agreement with the expected tumour suppressor function of SUFU. Finally, RNAs from one tumour could be profiled and demonstrated an expression pattern consistent with sonic hedgehog pathway activation.
Main characteristics of tumour cases
Discussion
The study of these two kindreds confirms the relevance of germline mutations of the SUFU gene in genetic predisposition to medulloblastoma. In the report published by Taylor,5 truncating mutations of the SUFU gene were found in 4/46 cases of desmoplastic medulloblastoma and were associated with deletions or mutations of the wild type allele. As in Taylor's report, the two mutations identified in our study are frameshift mutations leading to a premature termination of the RNA. These two mutations involve a seven nucleotide long C stretch located in exon 1 with a deletion of a C in one family and an insertion in the other family. The presence of DNA variants within this polyC stretch was not observed in 70 independent healthy patients. It was observed only once within 116 DNAs from sporadic medulloblastomas. In this last case, the mutation was different from the two described here. It was a deletion of two C with insertion of a T (c.65_66delinsT). It concerned a desmoplastic/nodular medulloblastoma in a 10-month-old child. No constitutional DNA was available to document a putative germline mutation. These results indicate that no recurrent polymorphism of this C stretch is found and that all variants of this sequence can be pathogenetically related to the occurrence of medulloblastoma.
Another striking finding of this study is the occurrence of three cases of the MBEN subtype in these two kindreds. The association of such cases with germline SUFU mutations underlines the implication of the sonic hedgehog pathway in the pathogenesis of this rare subtype, accounting for only 1–2% of all medulloblastoma cases. That one case of MBEN and two cases of typical nodular/desmoplastic medulloblastoma are associated in the same family confirms the pathogenetic relationship between the two entities.
Medulloblastoma was diagnosed in all seven patients before 3 years of age and in four patients during the first year of life. We cannot exclude the possibility that the other tumour cases observed in SUFU mutation carriers (a breast cancer at 37 years, a meningioma at 38, and a leiomyosarcoma at 63 years) may somehow be related to this mutation. However, apart from the first years of life, the risk of cancer associated with germline SUFU mutations does not appear to be particularly high. Penetrance was estimated through the proportion of carriers among unaffected individuals excluding obligate carriers who are less likely to be affected, which corrects for the ascertainment bias through several affected individuals.11The penetrance was estimated to be 30%. We cannot evaluate whether the incomplete penetrance observed here is linked to the position of the two mutations within exon 1, possibly allowing transcription of an almost complete protein from putative cryptic promoters, or whether it constitutes an intrinsic characteristic of familial medulloblastomas linked to SUFU mutation. If the latter is the case, yet unidentified modifier genes or environmental factors may play a crucial role. Interestingly enough, close to half of the individuals who inherited the mutation from their mother developed a medulloblastoma (8/17), whereas none of the carriers who inherited the mutation from their father developed the tumour (0/4). This suggests that parental imprinting may play a role in the tumorigenesis and partly explains incomplete penetrance in this context. Nevertheless, it should be emphasised that SUFU is not a known imprinted gene and that the present bias in parental transmission has to be confirmed in other series.
Familial aggregations of medulloblastoma are rare,7 8 suggesting that the incidence of these inherited germline mutations is low. However, we cannot exclude the possibility that some cases of apparently sporadic medulloblastoma may be associated with de novo mutations of the SUFU gene.
In conclusion, our report highlights three important features of SUFU related tumours. First, these are mainly, if not exclusively, MBEN or typical desmoplastic/nodular medulloblastomas. Secondly, these tumours mostly, if not exclusively, appear during the first 3 years of life. Finally, the penetrance of the mutation is incomplete and the role of non-Mendelian inheritance modes needs to be further evaluated.
Acknowledgments
Thanks to Veronique Byrde, Bénédicte Thuille, Stéphanie Reynaud and Catherine Bonaïti, for fruitful discussions and technical assistance and Lorna Saint Ange for editing. This work was supported by grants from the Ligue Nationale Contre le Cancer (Equipe Labellisée). We also wish to thank the association Trajectoire.
Footnotes
Funding Other funders: Ligue Nationale Contre le Cancer, Paris, France.
Competing interests None.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.