Article Text

Abstract
Silver–Russell syndrome (SRS) is a clinically heterogeneous disorder characterised mainly by intrauterine and postnatal growth retardation. While maternal uniparental disomy of chromosome 7 is found in 5–10% of SRS patients, recently genetic and epigenetic mutations affecting the imprinting centres on chromosome 11p15 have been reported in up to 64% of patients. Chromosome 11p15 abnormalities reported in SRS include methylation defects in the imprinting centre 1 (ICR1) and maternally inherited duplications involving all or part of the imprinted region of 11p15. Here we report the first published case of SRS with mosaic maternal uniparental disomy of chromosome 11.
Statistics from Altmetric.com
Silver–Russell syndrome (SRS) (OMIM 180860) is characterised by intrauterine and postnatal growth retardation. Other features include relative macrocephaly, triangular face with a prominent forehead, body and limb asymmetry, clinodactyly and feeding difficulties.1 2 Maternal uniparental disomy (UPD) of chromosome 7 (mUPD7) is present in 5–10% of SRS patients.3 However, epigenetic and genetic mutations affecting the imprinted gene cluster on chromosome 11p15 have now been implicated in a majority of cases. The telomeric imprinting domain imprinting centre 1 (ICR1) (IGF2/H19DMR, DMR1) regulates expression of the maternally expressed H19 and the paternally expressed IGF2 genes. Normally ICR1 is methylated on the paternally inherited allele but hypomethylation has been reported in up to 64% of patients with SRS.4–7 Recently, the centromeric imprinting centre ICR2 (DMR2, KvDMR) was also implicated by the finding of a patient with SRS and a maternally inherited cryptic duplication that includes ICR2 but not ICR1.8 ICR2 is normally methylated on the maternally inherited allele and regulates the expression of several genes, including the maternally expressed KCNQ1 and cell cycle regulator CDKN1. Maternally derived duplications of 11p, including both ICR1 and ICR2, have been previously identified in three growth retarded patients9 and, more recently, seen in two of 46 SRS patients.10
The imprinted gene cluster on 11p15.5 is also involved in Beckwith–Wiedemann syndrome (BWS), an overgrowth syndrome—the epigenetic alterations seen in SRS so far are the opposite of those seen in this syndrome. Among the known causes of sporadic BWS are: hypermethylation of ICR1 (2–7%), hypomethylation of ICR2 (∼50%), mosaic paternal UPD (∼20%), and paternally inherited duplications of the region (<1%). Hitherto, maternal UPD of chromosome 11 (mUPD11) has not been described in a patient with SRS. Here we report a patient with SRS caused by mosaic mUPD11.
CASE REPORT
The proband was the first child of healthy, non-consanguineous parents. At 13/40, the expected date of delivery was revised according to measurements on ultrasound scan, though her mother was confident of the date of her last menstrual period. A routine anomaly scan at 20 weeks identified a cleft palate and the abdomen was noted to be relatively small in comparison to head size. Subsequent scans confirmed poor fetal growth but Doppler ultrasound scans showed no evidence for placental insufficiency. Amniocentesis showed a normal female karyotype.
She was born at 37 weeks gestation with a birth weight of 1.76 kg (0.4th centile). Subsequently her growth remained parallel to, but below, the 0.4th centile. She was first seen in the genetics clinic at 6 months, at which time a diagnosis of SRS was considered. She had a cleft palate repair at 8 months. From birth she had severe feeding difficulties and at 14 months a gastrostomy feeding tube was inserted as her weight was static on nasogastric feeds. She was also noted to sweat profusely, especially in infancy.
At 2 years 6 months she had mild gross motor delay but otherwise her cognitive development, including speech development, was in the normal range. Her height was −4.5 SD, weight on the 0.4th centile, and head circumference on the 75th centile. She was noted to have a triangular facial appearance with frontal bossing and mild facial asymmetry. She had no limb asymmetry and slight fifth finger clinodactyly.
Initial investigations showed a normal female karyotype. 22q11 FISH (fluorescence in situ hybridisation) analysis, performed in view of the cleft palate, detected no abnormality. Maternal UPD7 was excluded. She was subsequently referred for methylation analysis of the H19/IGF2 region in 11p15.5.
METHODS
DNA was extracted by standard methods from peripheral blood and a mouth brush sample. This was analysed for methylation abnormalities of ICR1 and ICR2, for duplications or deletions of 11p15, and for UPD of chromosome 11.
In preparation for methylation specific polymerase chain reaction (MS-PCR), 2 μg DNA was bisulfite treated using the EZ methylation kit (Zymo research, Orange, California, USA) and recovered in a final volume of 50 μl. MS-PCR utilises the divergent sequence changes arising from bisulfite treatment of differentially methylated DNA, yielding differently sized amplicons in a ratio reflecting that of the starting material. MS-PCR analysis of both ICR1 and ICR2 was performed as detailed previously.11 12 Each PCR was done in triplicate on patient DNA from two independent bisulfite treatments, together with positive (Amsterdam, The Netherlands) and normal (n = 4) controls from the same bisulfite treatment.
Multiplex ligation dependent probe analysis (MLPA) and methylation sensitive MLPA (MS-MLPA) of the 11p15 region utilised the ME030 kit from MRC-Holland (Amsterdam, The Netherlands) and was performed according to the manufacturer’s instructions.
Microsatellite repeat analysis was performed using 24 primer sets located from 11p15.5 to 11q24.2, with standard PCR conditions and 27 cycles of replication. PCR products were visualised using an ABI 3100 DNA analyser. The ratio of peak height of upper allele: peak height of lower allele was calculated for all heterozygous results, enabling a comparison to be made between ratios from the proband and those of her parents at the same loci.
DNA obtained from the mouth brush sample was not of sufficient quality or quantity for use in MS-PCR and microsatellite repeat analysis.
RESULTS
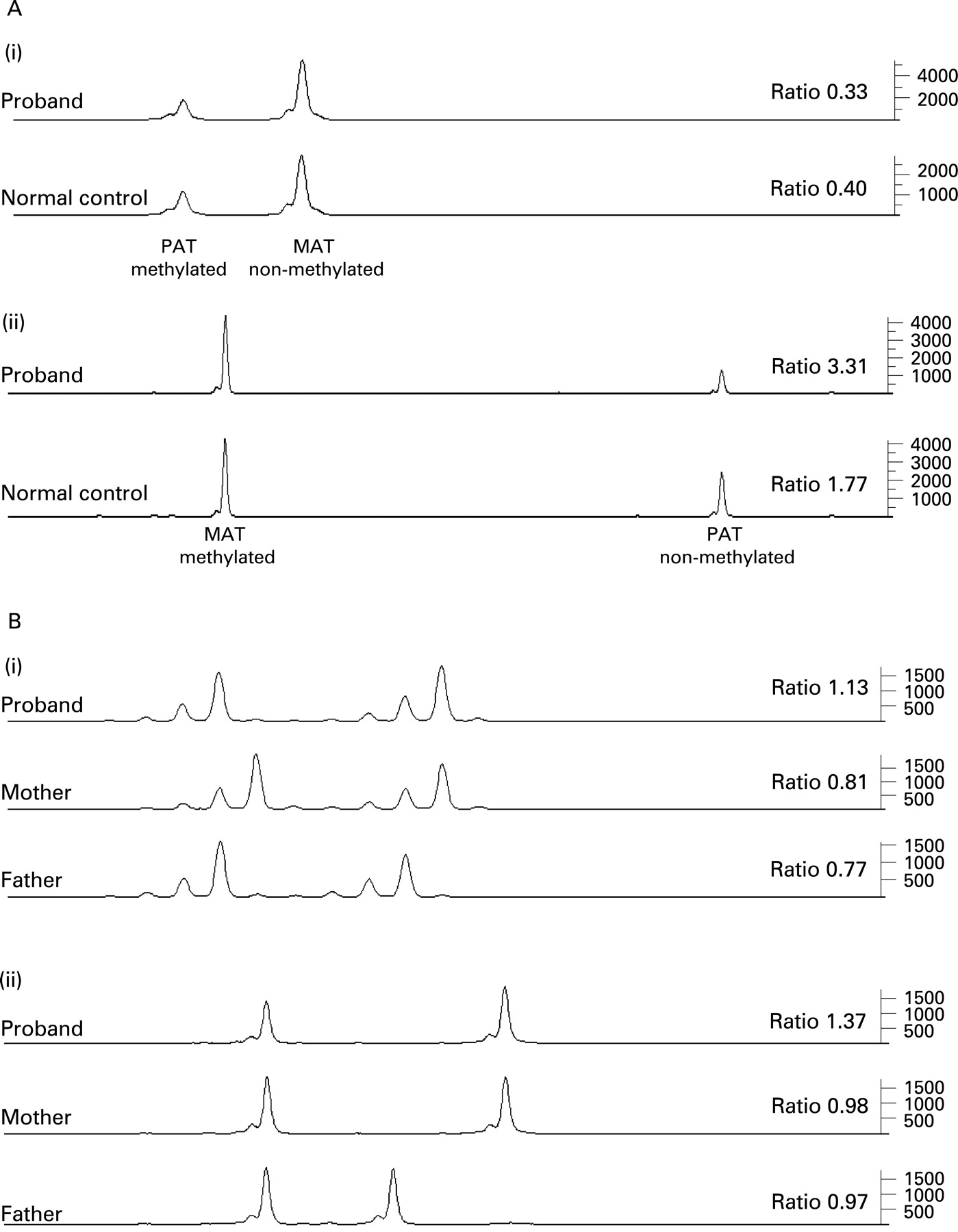
MS-PCR analysis at ICR1 gave a ratio of methylated: non-methylated alleles of 0.75 times the average of the within assay normals, a borderline normal result. However, analysis of ICR2 yielded a convincingly abnormal ratio of approximately 1.7 times the normal average (fig 1A). In this laboratory MS-PCR results of 0.85–1.2 are considered normal while those below 0.6 and above 1.5 are considered abnormal. Borderline cases will require further analysis.
{kind=link}
MLPA analysis detected no alteration of copy number, indicating that no duplication or deletion of the region was present. No methylation abnormality was visible with the initial MS-MLPA reactions performed. However, a later version of the ME30 kit, containing additional probes, showed a slight loss of methylation at ICR1 and gain of methylation at ICR2 with both the blood and mouth brush samples (data not shown).
Of the 24 primer sets used to amplify microsatellite repeats, 12 were fully informative and comparison between the peak height ratios (upper/lower alleles) obtained from the proband and the equivalent ratio from her parents showed an increased dosage of the maternally derived allele, indicating either mosaic mUPD11 or a mosaic maternally derived duplication. The MLPA result had excluded a copy number change, therefore this result is indicative of mosaic mUPD11. All the other loci examined gave results consistent with mosaic mUPD11. The 12 informative loci were located from 11p15.5 to 11q23.3 (table 1, fig 1B). There was no evidence of a third allele at any of the loci examined.
At those loci where a parent has alleles identical to the patient, it is possible to obtain an estimate of the degree of mosaicism by comparing the ratio of peak heights from the proband with that from the parent. Results from eight loci were suitable for this calculation which revealed that the maternally derived allele was on average 1.37 times higher than would be expected. This suggests the presence of an isodisomic cell line with an estimated level of mosaicism of 18%.
DISCUSSION
Genetic and epigenetic anomalies involving the imprinted gene cluster on 11p15 have recently been recognised as a cause of SRS. Put simply, SRS is associated with gene anomalies opposite in nature to those seen in BWS—for example, hypomethylation (SRS) versus hypermethylation (BWS) of ICR1, and maternal (SRS) versus paternal (BWS) duplications of 11p15. In keeping with this pattern, our finding of mosaic, apparently whole chromosome, maternal isodisomy of chromosome 11 is the reciprocal of the mosaic paternal isodisomy seen in BWS. Mosaic pUPD11 is seen in approximately 20% of BWS patients and of these the majority are segmental isodisomy of varying lengths, with only about 8% having pUPD of the whole chromosome.13
It is noteworthy that until now no case has been reported with mUPD11 and SRS, and that the degree of mosaicism in this patient was such that it was at the limits of detection by MS-MLPA and gave a borderline result at ICR1. Although ∼20% of sporadic BWS cases are caused by mosaic pUPD11 and ∼50% by hypomethylation of ICR2, there is apparently a strikingly low prevalence of SRS caused by anomalies involving ICR2. It may be that mosaic mUPD11 is a more common cause of SRS than is currently apparent, but it is difficult to detect, either for technical reasons or because it frequently involves tissues other than the lymphoblastoid cells sampled for testing. Alternatively, it may be that anomalies involving increased maternal dosage of ICR2 are uncommon in SRS, perhaps because the resultant gene expression in some tissues is incompatible with life.
The current improvements in the sensitivity of DNA methylation assays should allow identification of the molecular cause in further SRS cases enabling any phenotype/genotype correlations to emerge. Testing of DNA from tissues other than blood may also prove to be diagnostically valuable.
REFERENCES
Footnotes
Competing interests: None declared.
Patient consent: Parental informed consent was obtained for publication of the patient’s details in this report.