Article Text

Abstract
Maternal uniparental disomy for the complete long arm of chromosome 14 has been reported in 14 patients to date and is associated with a specific pattern of malformation. We report a child with clinical features of this syndrome who exhibits maternal uniparental disomy confined to a specific interstitial segment of chromosome 14.
- maternal uniparental disomy
- chromosome 14
- imprinting
Statistics from Altmetric.com
A specific pattern of malformation is associated with maternal uniparental disomy 14 (UPD(14)mat), which is distinct from that seen with paternal uniparental disomy 14 (UPD(14)pat). Intrauterine growth retardation (IUGR), developmental delay, premature puberty, hypotonia/joint laxity, macrocephaly, short stature, and small hands are all characteristic of UPD(14)mat (table 1). Polyhydramnios, small thorax, rib defects, small ears, protruding philtrum, small palpebral fissures, and camptodactyly are found in subjects with UPD(14)pat.1 The differences in these phenotypes and the inheritance patterns suggest that this chromosome contains both maternally and paternally imprinted genes. All 14 UPD(14)mat patients reported to date appear to exhibit uniparental disomy for the complete long arm of this chromosome.2-15 In this paper we report a patient with UPD(14)mat confined to an interstitial segment of chromosome 14 (∼14q23-14q24.2) and discuss the probable origin of this event.
Major clinical features of maternal UPD(14) syndrome
Case report
The proband presented at the age of 3½ years for genetic evaluation secondary to developmental delay. She was born at term after an uncomplicated pregnancy with normal growth parameters. Her parents reported no problems at birth except for hypotonia. No records of her head size are available before 2 years of age, but at that time her OFC measured >98th centile. A subsequent head CT scan was normal. She sat at 8 months of age and walked at 15 months. By the age of 2½ years, concerns about her motor and speech delays led to formal developmental testing which indicated mild global developmental delay. Previous neurological and genetic evaluation showed global developmental delay, generalised hypotonia, macrocephaly, and joint laxity with a normal head MRI scan, normal karyotype, and normal DNA testing for the fragile X syndrome. On physical examination at 3½ years, her height was at the 25th centile, weight at the 10th centile, and head circumference above the 97th centile. No dysmorphic features were noted other than a slightly triangular face (fig 1). She continued to show generalised joint laxity. The possibility of UPD(14)mat was raised based on the triad of developmental delay, macrocephaly, and joint laxity, which are features characteristic of this syndrome.
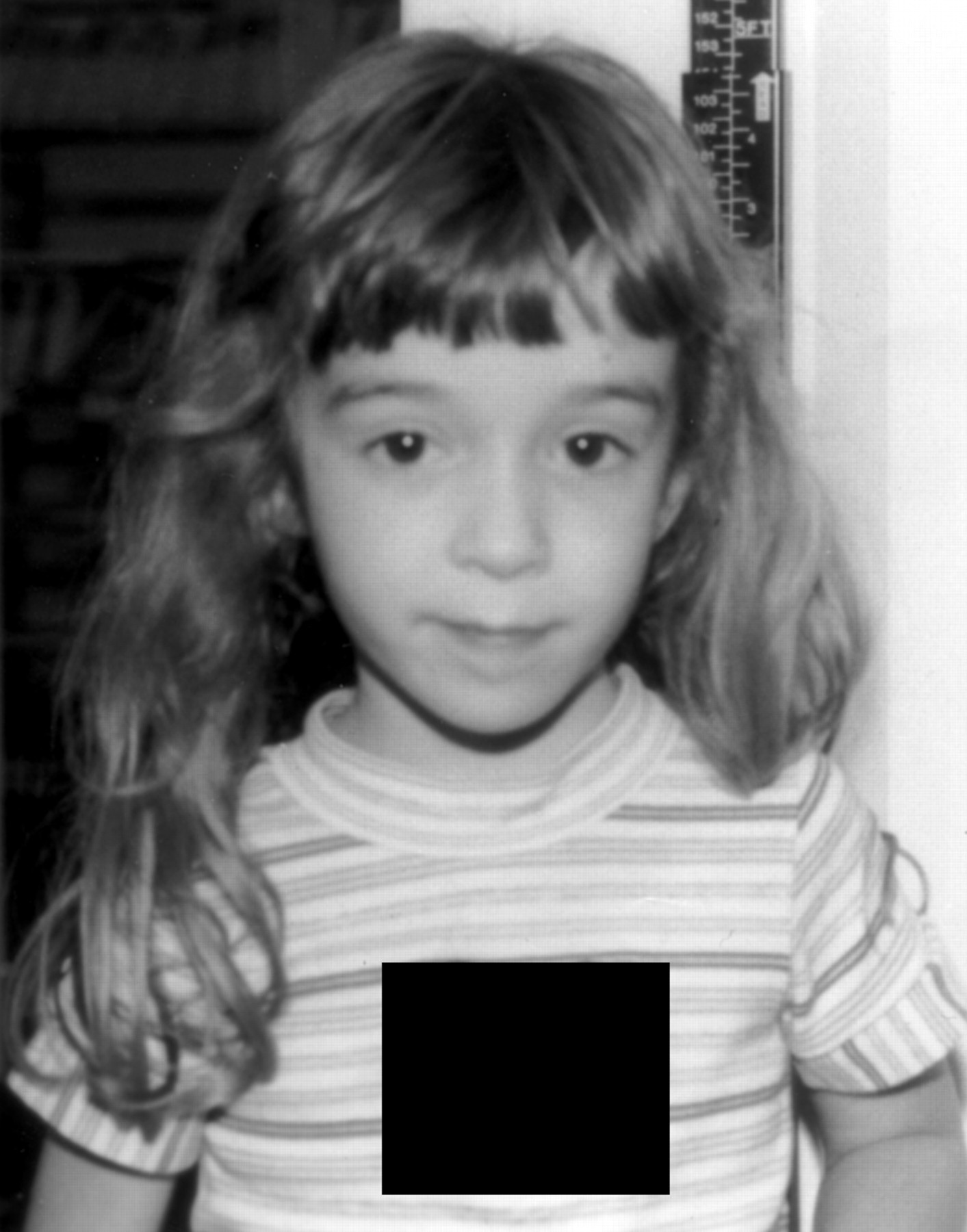
Front view of patient (photograph reproduced with permission).
Methods
Blood samples were collected from the patient and both of her parents. Genomic DNA was purified using a commercial kit (Gentra Systems, Minneapolis, MN) and inheritance at polymorphic chromosome 14 genetic loci was analysed routinely by PCR.16 The genetic markers (Research Genetics, Huntsville, AL) studied included D14S66, D14S63, D14S1002, D14S277, D14S268, D14S1028, D14S77, D14S61, D14S59, D14S74, D14S67, and D14S68. PCR conditions and genetic, cytogenetic, and physical map locations were obtained from the CEPH/Genethon and Marshfield genetic maps at the Genome Database (http://gdb.bioinfo.sickkids.on.ca/). PCR products were separated on denaturing polyacrylamide gels and visualised by exposure on autoradiography film.
Results
UPD(14)mat was observed at D14S277 and D14S77 was informative for heterodisomy (hetero-UPD(14)mat) (table 2, fig 2). D14S268, which maps between D14S277 and D14S77,17 was heterozygous and presumed to show heterodisomy (table 2). D14S66, which is proximal to these loci, and D14S1028, D14S61, and D14S67, which are distal, were biparentally inherited (table 2). In addition, markers D14S63 and D14S74 were found to be heterozygous, but the origin could not be determined owing to the presence of an allele shared by both parents. D14S68 was uninformative.
Genotypic analysis2-150

Autoradiographs of patient and parental genotypes at two loci that show UPD(14)mat.
Discussion
The maternal heterodisomic interval in this patient may be as small as 2 cM (the distance between D14S277 and D14S77) or as large as 21 cM (the distance between the flanking markers, D14S66 and D14S1028, displaying biparental inheritance). These genetic loci have been mapped to bands 14q23-14q24.2 (fig 3) and define the shortest genetic interval associated with the UPD(14)mat phenotype.

{kind=link}
{kind=link}
{kind=link}
Ideogram of chromosome 14 comparing locations of informative markers in previous reports of UPD(14)mat to those defining the maternal heterodisomy interval in this study. (Numbers across the top are reference numbers.) Cytogenetic assignments of markers have been interpolated from the physical assignments of adjacent anchor loci on genetic, physical, and chromosome maps.
The ideogram in fig 3 compares the regions of UPD(14)mat in our patient with nine of the 14 previously reported cases, for which details of genetic markers were available. This patient with UPD(14)mat is unique because maternal disomy is confined to an interstitial segment of chromosome 14q (rather than the complete long arm, as reported in previous cases). Complete UPD(14)mat results from either gamete complementation or a meiotic non-disjunction event involving a derivative chromosome (isochromosome 14 or a Robertsonian translocation) followed by trisomy rescue.18 Meiotic recombination may also ensue5 9 14 and generate both iso- and heterodisomic regions (fig 3). However, interstitial maternal heterodisomy confined between biparentally inherited loci also requires an early postzygotic recombination event to have occurred. In the present case, a mitotic double exchange first occurred between the paternal and one of two maternal chromosomes in a trisomy 14 zygote. This was followed by mitotic non-disjunction of the recombinant derivative chromosome containing the paternally derived interstitial segment.
Allelic mitotic recombination occurs more often than has been previously recognized.19-21 For example, between 20 and 28% of patients with sporadic Beckwith-Wiedemann syndrome show paternal isodisomy for the distal segment of chromosome 11p, felt to be the result of a single, rather than a double, postzygotic crossover event.22-24 Double mitotic recombination is also associated with loss of heterozygosity (LOH)19 25and has recently been suggested as a possible mechanism for leukaemia in patients with mutations in the NF1 gene25 and revertant mosaicism in epidermolysis bullosa.26 By contrast, the present case involves double reciprocal recombination without concomitant LOH.
Autosomal recessive inheritance has been suggested as an explanation for the UPD(14)mat phenotype based on previous observations of maternal isodisomy.4 However, autosomal recessive inheritance is unlikely because no consistent isodisomic interval exists between all of the cases reported to date (fig 3). Imprinting has also been suggested as the mechanism to explain the UPD(14)mat phenotype.1 27 Although no human genes in this region are yet proven to be imprinted,27 an imprinting effect is supported by studies in the mouse indicating that the distal portion of chromosome 12, recognised as a probable imprinted region,28 is syntenic with human chromosome 14q. Maternal origin effects based on studies of partial trisomy of chromosome 14q also suggest that 14q24.3-qter contains imprinted genes.27Paternally imprinted gene(s) have been localised to 14q22, based on transmission of an interstitial chromosome 14 duplication from a normal father to abnormal offspring.29 We propose that reciprocally imprinted genes are present within 14q22-q24.2, as has been found previously in 11p15.5 and in 15q11.2-q13.30 31
The extent of the disomic interval presented in this case should assist in refining the locations of imprinted genes associated with certain features found in UPD(14)mat syndrome. IUGR, short stature, and small hands have been seen in the majority of UPD(14)mat cases, but were not observed in our patient, suggesting that gene loci associated with their occurrence may be located outside the 14q23-14q24.2 region. Patients with partial trisomy 14q owing to maternal non-disjunction exhibit intrauterine growth retardation and small hands more frequently than those with trisomy resulting from paternal segregation errors.27 This common trisomy 14 interval is distal to the UPD(14)mat segment delineated in the current study. Finally, the occurrence of premature puberty (or lack thereof) in our patient, a consistent finding in other cases of UPD(14)mat, may facilitate localisation of imprinted gene(s) responsible for pathogenesis of this phenotype.
Note added in proof
Four additional patients with UPD(14)mat have recently been documented by Kotzot.32
Acknowledgments
Grant support is gratefully acknowledged from the Public Health Service (CA74683), the American Cancer Society (DHP-132), and the Merck Genome Research Foundation to PKR. We thank Dr Merlin Butler for his comments on the manuscript.
References
Footnotes
-
↵* Present address: Phylogenetix Laboratories Inc, 275 William Pitt Way, Pittsburgh, PA 15238, USA.