Article Text

Abstract
We report a study of 55 subjects with Smith-Magenis syndrome, aged 9 months to 35 years. Each person has been evaluated with an assessment of “gestalt” and detailed facial measurement, using previously published methodology, with compilation of Z score pattern profiles.
The facial phenotype of SMS is quite distinctive, even in the young child. The overall face shape is broad and square. The brows are heavy, with excessive lateral extension of the eyebrows. The eyes slant upwards and appear close set and deep set. The nose has a depressed root and, in the young child, a scooped bridge. With time, the bridge becomes more ski jump shaped. The height of the nose is markedly reduced while the nasal base is broad and the tip of the nose is full. The shape of the mouth and upper lip are most distinctive. The mouth is wide with full upper and lower lips. The central portion of the upper lip is fleshy and everted with bulky philtral pillars, producing a tented appearance that, in profile, is striking. With age, mandibular growth is greater than average and exceeds that of the maxilla. This leads to increased jaw width and protrusion and marked midface hypoplasia.
Craniofacial pattern analysis supports these subjective impressions. After mid-childhood, mandibular dimensions consistently exceed their maxillary counterparts. Craniofacial widths are greater than corresponding depths and heights. Nasal height is reduced while nasal width is increased. There is mild brachycephaly. The most marked age related changes are increased width of the nose and lower face (mandibular width) with reduction in nasal height and midfacial depth.
- Smith-Magenis syndrome
- facial measurements
Statistics from Altmetric.com
Smith-Magenis syndrome was first reported in 1982.1 It is associated with a deletion of chromosome 17p11.2. Since that time a distinctive somatic and behavioural phenotype has emerged.2-4 Short stature with small hands and feet are the norm. Scoliosis is frequently seen. There is a high likelihood of otorhinolaryngological complications, particularly deafness (sensorineural, conductive, or mixed) and vocal cord anomalies such as nodules and polyps, which contribute to a hoarse, low pitched voice. Ophthalmological differences, especially strabismus and myopia, are common. About one third of patients have a congenital heart defect, and in a similar proportion a genitourinary malformation, commonly a duplicated collecting system, is found. Hypothyroidism or immunoglobulin deficiency is documented in 20 to 25%.
It is the behavioural phenotype which is most distinctive. Aggression towards self and others is frequent, as is poor impulse control. The self-mutilation may take an unusual form such as onychotillomania, and may be related to the high tolerance of pain which accompanies this condition. Stress and excitement may be expressed as a characteristic behaviour known as auto-amplexation or self-hugging.5Self-stimulating behaviours are common. Sleep disturbance occurs with a variety of manifestations: difficulty getting to sleep, frequent waking, early rising, and reduced REM sleep.3 6
Recognition of the facial phenotype lags behind knowledge of somatic and behavioural manifestations, often contributing to delay in diagnosis. For this reason, a study of the face in Smith-Magenis syndrome was carried out by the authors using previously published methods.7
Materials and methods
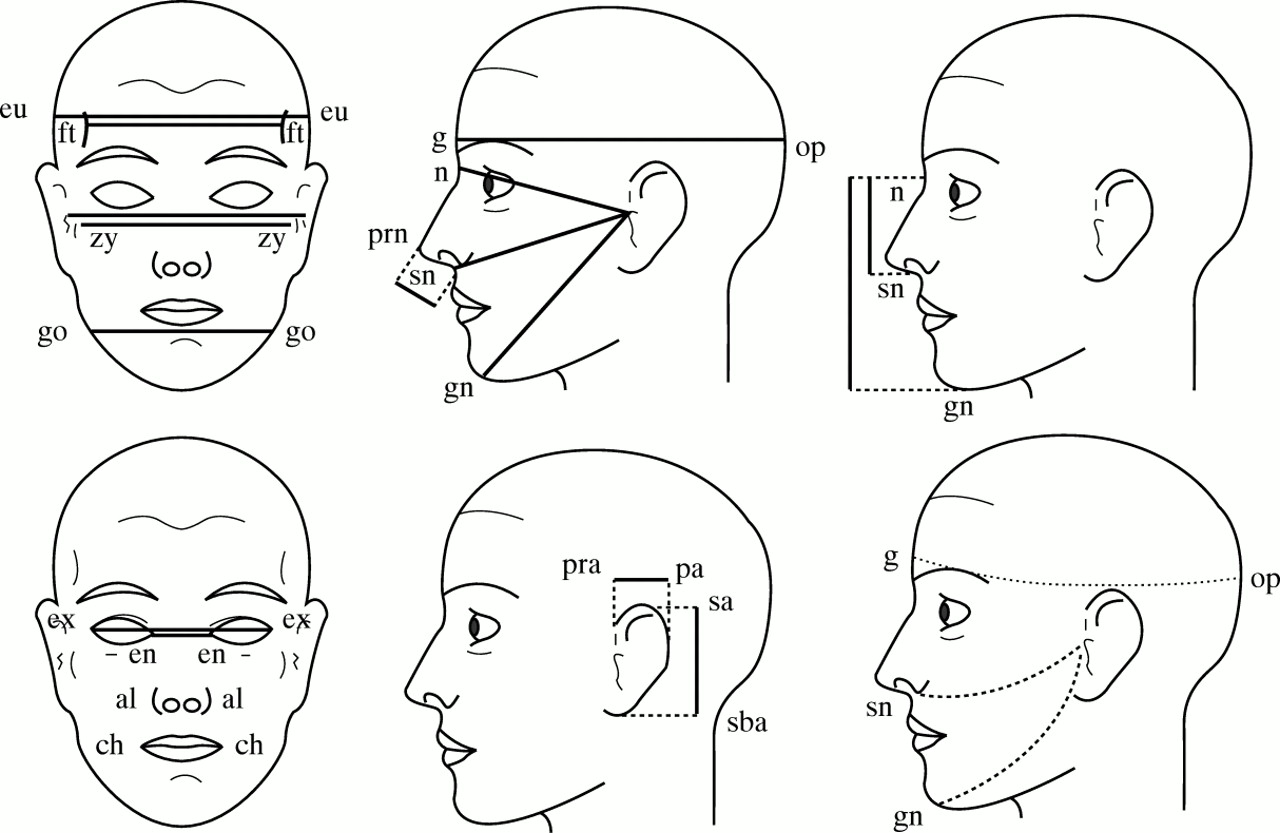
Fifty-five white subjects with Smith-Magenis syndrome (SMS) were ascertained through their physicians or the support group PRISMS, which held its first international meeting in 1997, at the National Institutes of Health. All persons with SMS were evaluated by a dysmorphologist familiar with the syndrome. In addition to an assessment of “gestalt”, a series of anthropometric measurements was obtained on each subject (table 1) following the method published by Farkas.8 Measurements were taken by one of the authors (JEA). They were recorded to the nearest 0.5 mm using GPM sliding and spreading, blunt ended calipers and a paper metric tape measure. These dimensions were chosen to represent craniofacial widths, lengths, depths, and circumferences plus details of ear, eye, nose, and mouth structure (fig 1). For each dimension, age and sex matched normal standards were available. The population norms were derived from measurements of the head and face in 2326 healthy North American white children and young adults.9 The raw data were compared to normal standards and converted to Z (standard deviation) scores to control for age and sex differences. Thus, a score of +1 would indicate a dimension one standard deviation above the mean. Pattern profiles were compiled for each age and sex. Because of small numbers at certain ages, additional profiles were produced for groups of subjects: ages 3 to 8, 8 to 12, 12 to 16, and 16 and over. Correlation coefficients and variability indices were generated by the Statistical Package for Social Scientists (SPSS), using the methods published by Garnet al. 10 11
Anthropometric measurements used in this study
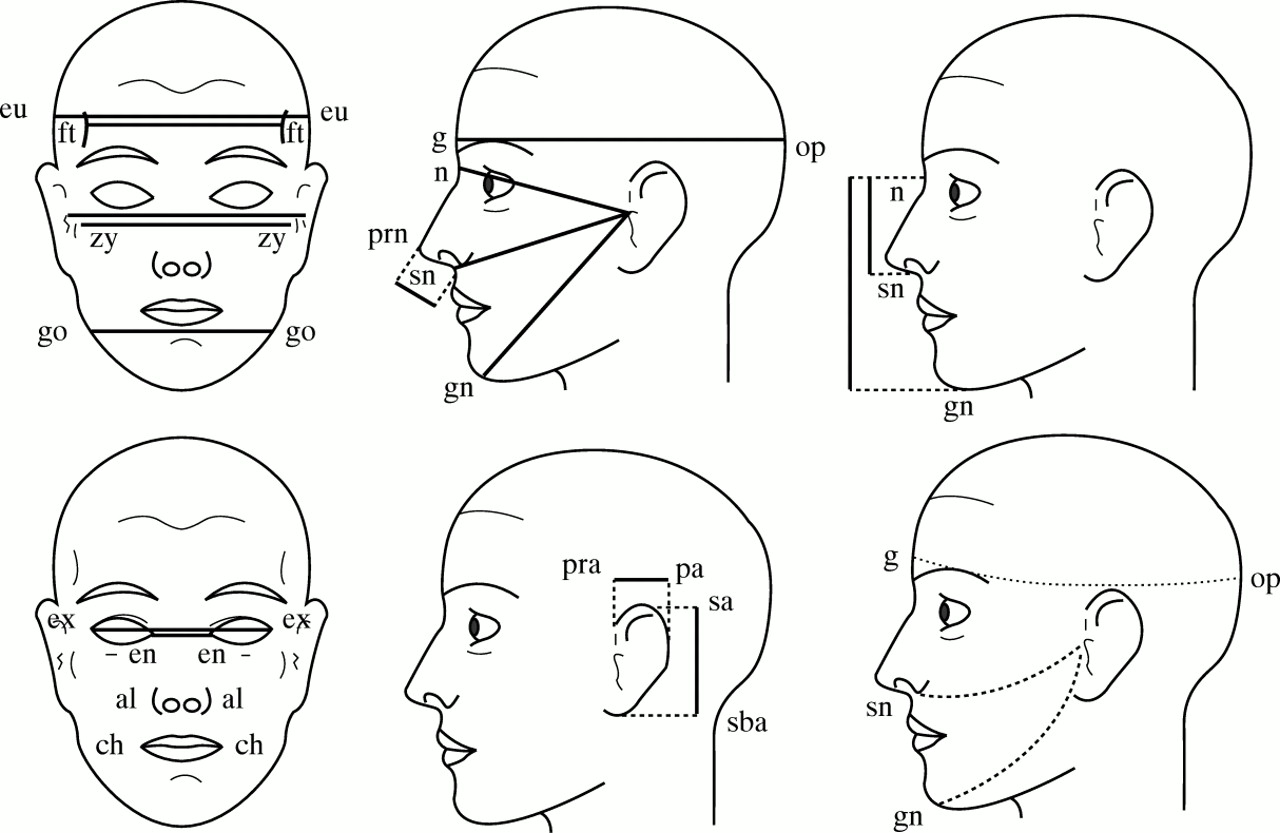
Craniofacial dimensions used in this study (also used in J Med Genet 1997;34:645).
Results
The subjective component of this study provided the following data. The characteristic face of Smith-Magenis syndrome is round or square with a flattened midface. The eyes slant upwards and are relatively close set. The brows are heavy and contribute to the impression that the eyes are deep set, particularly in the young child, when the eyes are usually the most prominent feature of the face. The nose is short with a broad base and full tip. Nasal height is markedly reduced. It is the upper lip which is most distinctive. The mouth is broad with full upper and lower lips. The central portion of the upper lip is fleshy and everted with bulky philtral pillars, producing a tented and strikingly protuberant appearance such that, in profile, the lip outline is parallel to the nasal bridge. Hair and skin colouring is generally fair or blonde, although eyebrows and lashes may be darker (figs 2 and 3). With increasing age, the face lengthens, as seen in the general population. There is striking broadening of the lower jaw, increasing the squareness of the face, with associated prognathism. Midface flattening is accentuated. The brows may become even heavier and almost pugilistic in character. They extend further laterally than normal and may have an upward slant (fig4).

The face of a infant with Smith-Magenis syndrome. (All photographs reproduced with permission.)

The face in mid-childhood.

An adult with Smith-Magenis syndrome.
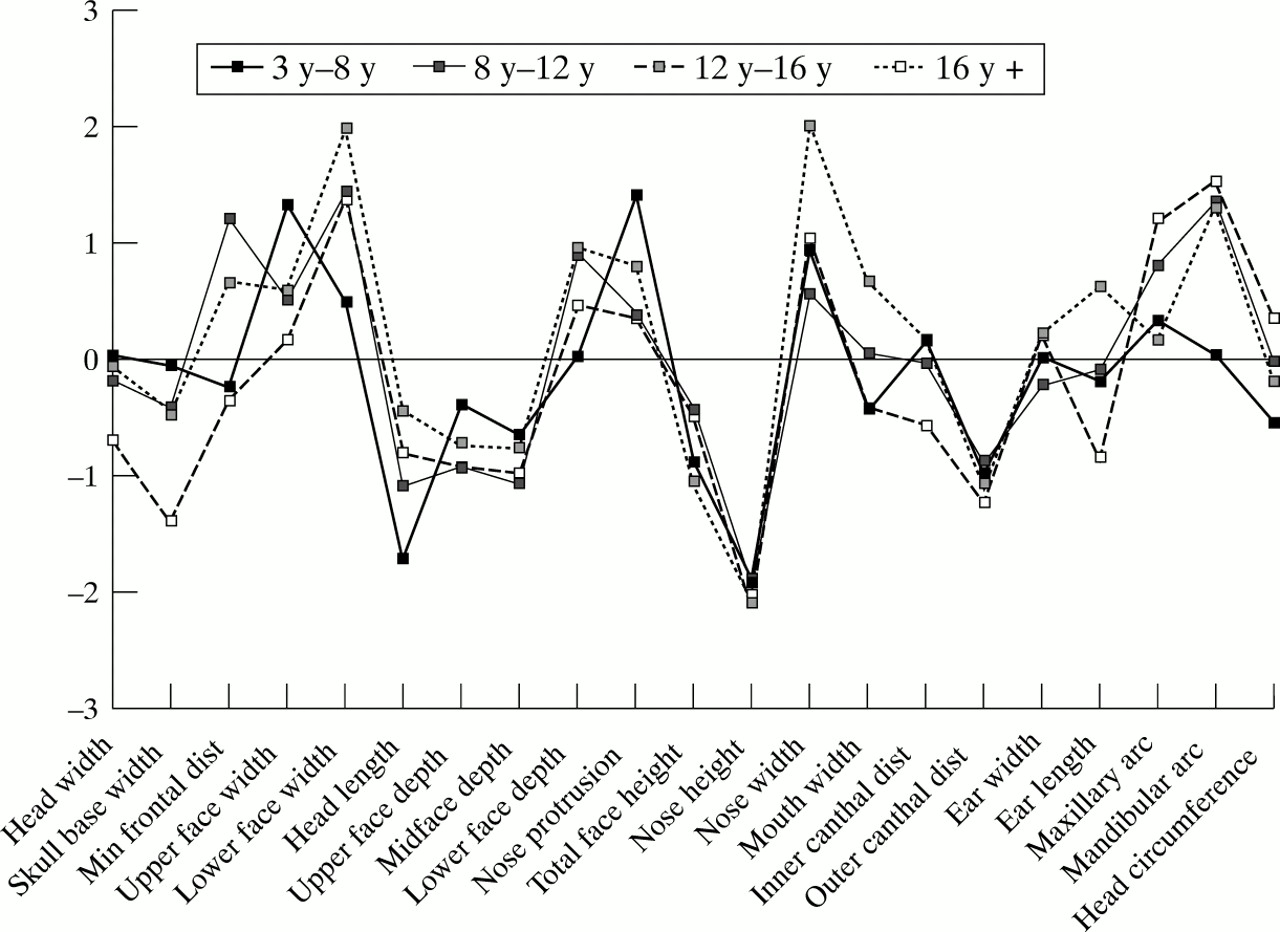
Anthropometric analysis is shown in fig 5. Four patterns representing different age groups are seen. There is considerable similarity between patterns. Table 2 documents the correlation between age groups. The closest correlation is between groups 1 and 2, and 2 and 3 (p<0.001). Group 4 is less closely correlated with other groups (p<0.01). When the degree of dysmorphogenesis (that is the variation from the mean) is evaluated, the group aged 12 to 16 are most discrepant from average, with a variability index of 1.04, while the oldest group, aged 16 and above, has the least discrepant pattern, with a variability index of 0.55.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Anthropometric pattern profile comparing four groups of subjects. Note the high concordance between patterns, with principal differences seen in the group aged 3 to 8 (thick line), where maxillary dimensions exceed their mandibular counterparts.
Correlation coefficients
The head circumference is normal with mild brachycephaly (head length less than head width). Craniofacial widths exceed normal while depths are less than the mean, which validates subjective impressions of a wide face with midface flattening. Nasal height is reduced while nasal width and protrusion are increased. Mandibular dimensions exceed their maxillary counterparts in all age groups except the youngest (age 3 to 8). In this age range, maxillary widths and circumferences are greater than those of the mandible. This suggests that the dominance of the mandible, producing the square and protruding jaw, is not present early but arises by mid-childhood.
Discussion
Smith-Magenis syndrome (SMS) has a characteristic facial appearance which is seen at all ages, but which becomes most obvious by mid-childhood. Previous reports have drawn attention to the presence of brachycephaly (95%), midface hypoplasia (95%), broad face (90%), broad nasal bridge (80%), downturned corners of the mouth (60%), frontal bossing (60%), prognathism (60%), telecanthus (60%), and upward slanting palpebral fissures (45%).2 Familiarity with the behavioural features clearly exceeds recognition of the facial phenotype. This has led frequently to delay in diagnosis. Fortuitous early diagnosis may occur at birth or in infancy, when unusual features suggest a diagnosis of Down syndrome, leading to a request for chromosome analysis which shows the 17p deletion. This phenotypic overlap with Down syndrome, particularly early in life, can be striking. Both conditions share brachycephaly, upward slanting palpebral fissures, a short and broad nose, a round face with midface flattening, iris hamartomas (Brushfield spots in Down syndrome and Wolfflin-Kruckmann spots in SMS), small size, small hands and feet, and hypotonia.
This study was initiated to draw attention to the most significant and consistent facial features in order to facilitate early clinical diagnosis. A subjective and objective approach was chosen since the two techniques are complementary. An assessment of “gestalt” can teach the observer about component parts but better appreciates the whole face, facial proportions, and relationships. Anthropometric assessment can highlight facial dimensions which are most different from normal and those closest to the mean, training the eye to appreciate the features which best represent the syndrome and discriminate it from other syndromes with which it overlaps. This technique can also validate subjective impressions. Anthropometry is a simple, non-invasive assessment which, in the cooperative child or adult, takes little time. However, the necessary skills require training and practice, and appropriate instrumentation is fairly expensive. For these reasons, the technique is used mainly as a research tool.
In conclusion, Smith-Magenis syndrome displays a characteristic facial phenotype. Familiarity with the clinical manifestations should improve the likelihood of early diagnosis and intervention. We have shown that particular craniofacial features facilitate syndrome identification, including a bulky and everted upper lip, deep set and relatively close set, upward slanting eyes, a short broad nose, midface hypoplasia, and a broad, protuberant lower jaw. Facial dysmorphism evolves over time and is more subtle in early childhood. The mandibular dominance, a striking component of phenotype recognition, only develops in mid-childhood. Age also enhances the somewhat coarse appearance of the face. Subjective and objective data are highly concordant. However, in young adults with SMS the pattern of features is least discrepant compared to the mean, despite the fact that, subjectively, the phenotype is well developed and striking by this age. This finding may highlight one of the inherent distinctions between overall “gestalt” and scrutiny of individual dimensions.
Acknowledgments
We are grateful for the cooperation of many families and the support group PRISMS. Drs Montgomery, Webber, Udwin, Donaldson (UK), and Yurenka, Weksberg, and Farrell (Canada) were particularly helpful in facilitating patient contact. This research was supported by the Medical Genetics Branch, National Human Genome Research Institute, National Institutes of Health, USA.