Article Text

Abstract
We report on a female fetus of 24 weeks whose clinical and radiological findings were compatible with boomerang dysplasia (BD). However, histopathology was unusual with a lateral fan shaped diaphyseal ossification. This has never been described either in typical atelosteogenesis I (AT-I) or in BD. The purpose of this report is to find out if this condition is a separate lethal bone dysplasia or another histological feature of the nosological group of AT-I and BD.
- boomerang dysplasia
- atelosteogenesis
- lethal chondrodysplasia
- lethal dwarfism
Statistics from Altmetric.com
Boomerang dysplasia (BD) is a lethal chondrodysplasia which was first reported by Kozlowskiet al 1 as a “new form of neonatal death dwarfism”. Three further male cases were documented by Tenconi et al,2 Kozlowskiet al,3 and Winshipet al.4 The characteristic flat, curved shape of one or more of the long bones gives this syndrome its name. Hunter and Carpenter5 and Greallyet al 6 suggested that BD and atelosteogenesis I (AT-I) may represent part of a spectrum of bone dysplasias with a possible common cause. Recently, Sillenceet al 7 reported a review of 25 cases of “atelosteogenesis syndromes” including seven other cases of BD.
The present case may be an early form of BD with characteristic radiographic features but in a female fetus and with an unusual diaphyseal ossification.
Case report
CLINICAL FINDINGS
A female fetus was medically aborted at 24 weeks of gestation. It was the first pregnancy of a 23 year old mother and a 26 year old father, both healthy and non-consanguineous. The gestation was complicated by polyhydramnios at 22 weeks and ultrasound study showed a marked shortness of the fetal long bones with abnormally shaped femora and mildly decreased ossification of the skull. The findings were interpreted as possible osteogenesis imperfecta. On amniocentesis, the karyotype was normal (46,XX).
External examination (fig 1) showed a 510 g (normal for dates) female fetus with macrocephaly, a large anterior fontanelle, hypertelorism, elongated philtrum, and micrognathia. The palate was intact.

External examination of the fetus was remarkable for severe micromelia, broad and short hands and feet (A, B), macrocephaly, hypertelorism, elongated philtrum, micrognathia (C), and talipes equinovarus (D).
There was an overall and symmetrical shortness of the four limbs. The elbow joints could not be seen. The hands and feet were broad and short, the abdomen was protuberant, and there was a bilateral equinovarus deformity. The internal organs were normal.
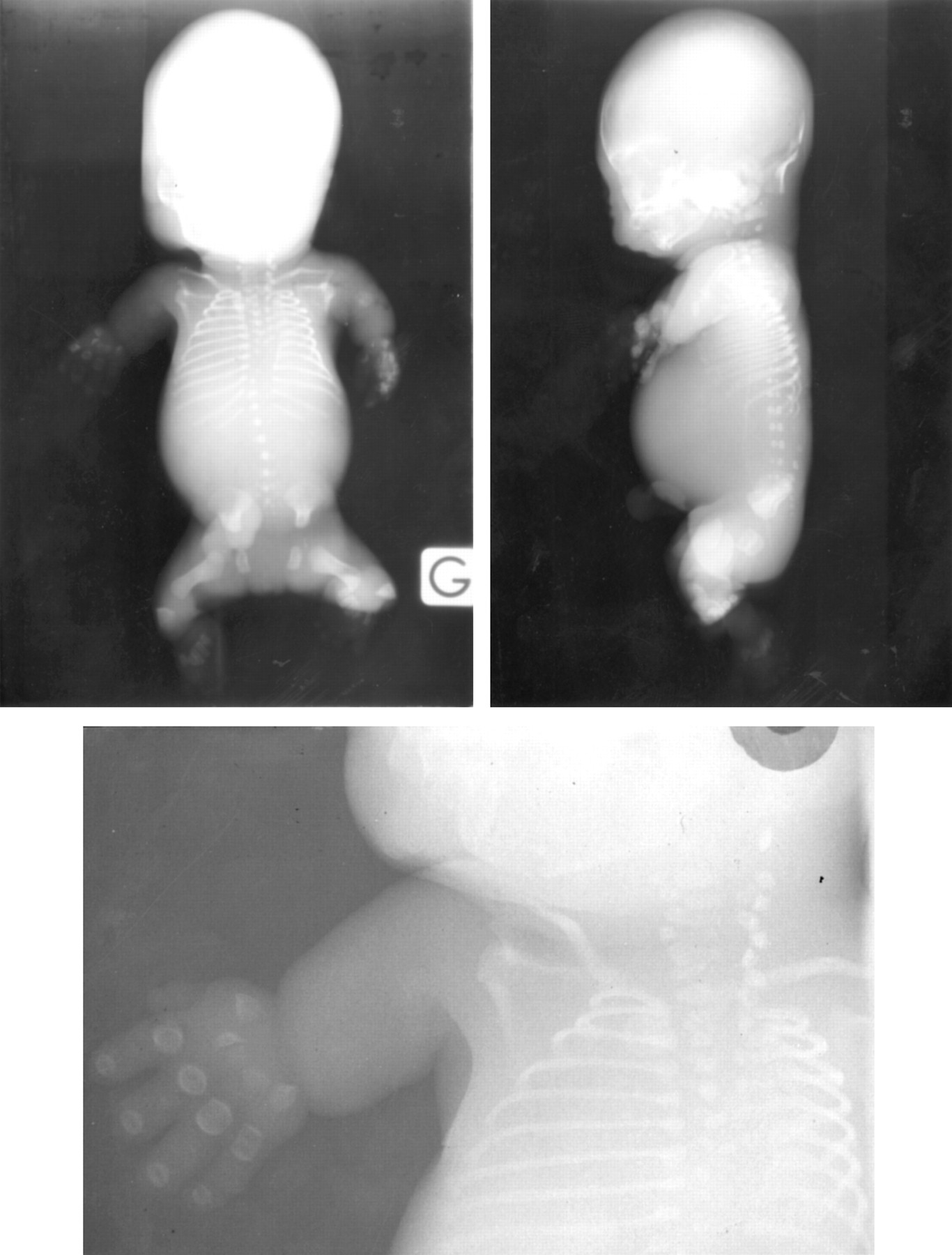
RADIOGRAPHIC FINDINGS
The radiographic study (fig 2) showed delayed ossification of the spine which was dysplastic. The thorax was narrow with 12 pairs of ribs. The iliac wings were triangular. Complete absence of ossification was noted in the humerus, radius, and ulna, except for one irregular ossification centre in the left upper limb. There were short ossification centres of some metacarpals and only the proximal and distal phalanges were ossified and wide. The femora were markedly short and curved. There was a triangular ossification centre instead of the tibia and fibula. Study of the feet showed irregular ossification of the metatarsals and only the distal phalanges were ossified.

Postmortem radiograph of the 24 week fetus illustrating delayed ossification of the spine, triangular iliac wings, absence of ossification in the humerus, radius, and ulna, markedly short femora, well ossified but dysplastic metacarpals and metatarsals, and an unusual ossification pattern of the phalanges.
HISTOPATHOLOGY
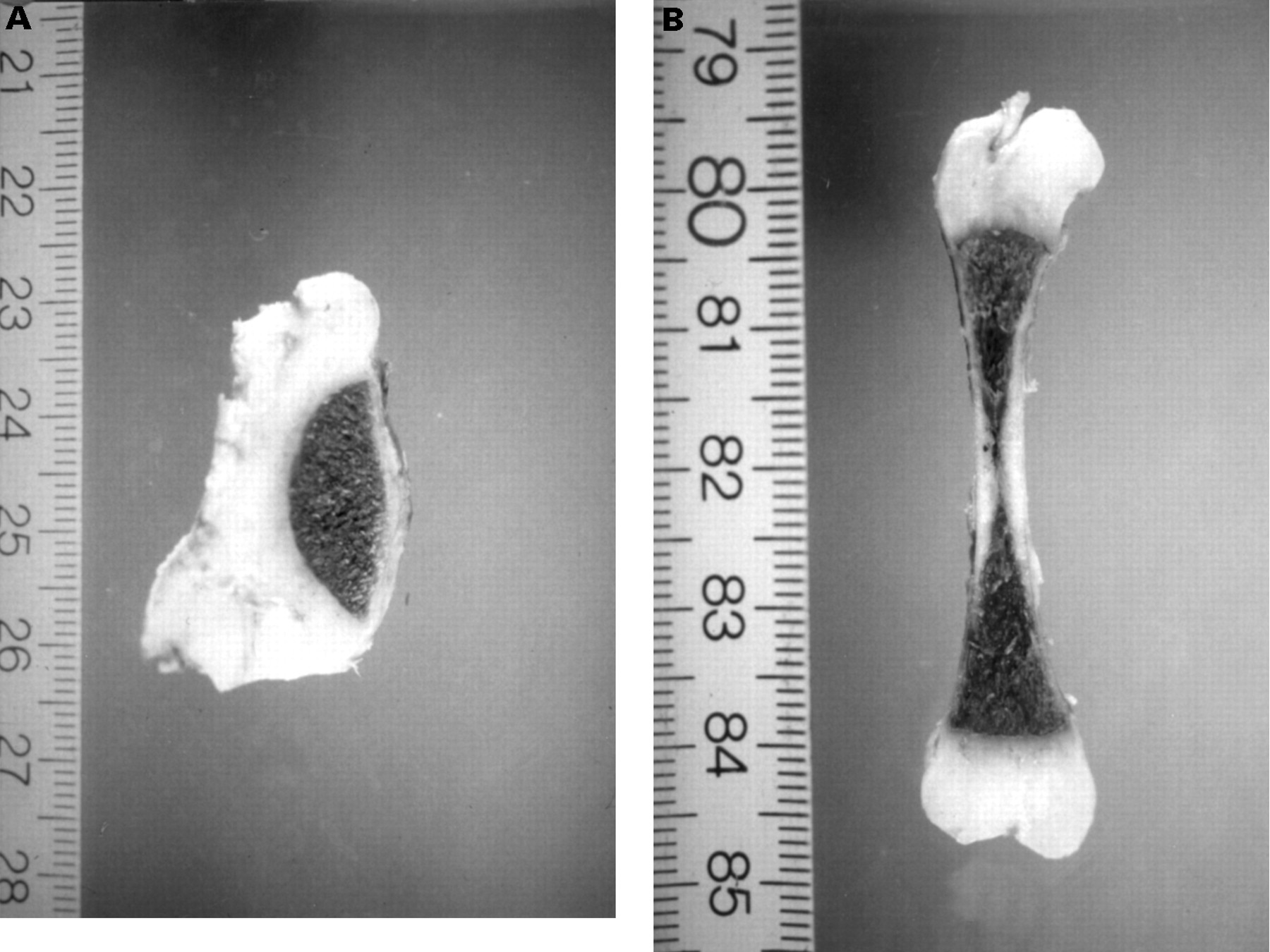
The femora were markedly short (length 35 mm) and wide (width 17 mm). The frontal section showed an unusual and fan shaped diaphyseal ossification (fig 3). This fan shaped ossification indicated hemispherical ossification with a vertical diameter on one diaphyseal side.

(A) Frontal section of the femur showing lateral fan shaped diaphyseal ossification. (B) Control : a normal femur at 24 weeks of gestation.
The specimens were embedded in paraffin after decalcification; sections were stained with H&E, PAS, alcian blue, and trichrome.
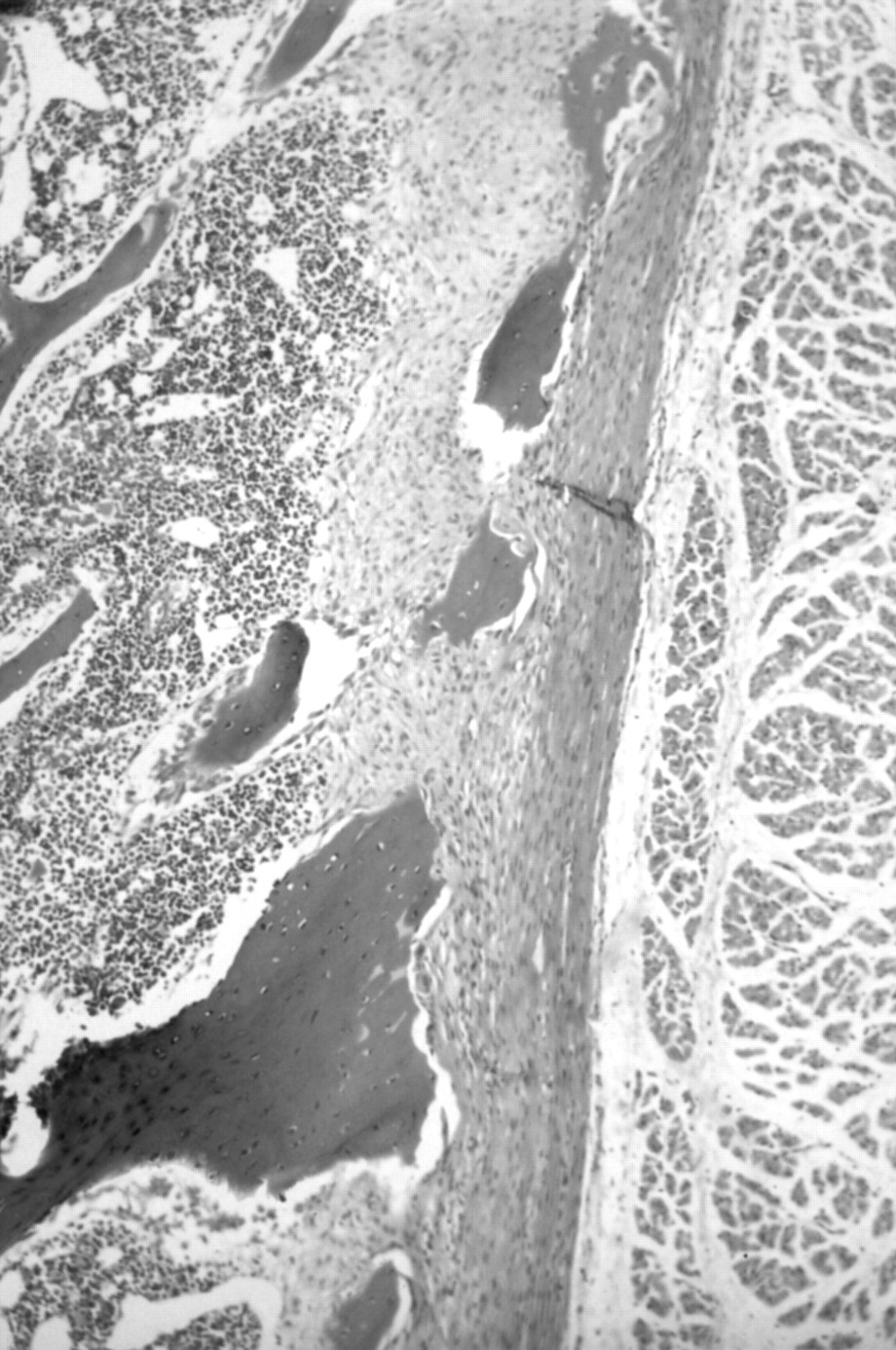
Microscopic examination confirmed an unusual distribution of the endochondral ossification (fig 4). In the resting cartilage, there was an abundant matrix with scattered, large chondrocytes. In the physeal growth zone there were many irregular vascular canals which disturbed the columnar arrangment of the chondrocytes in the proliferative and hypertrophic zones (fig 5). The hypertrophic chondrocytes were quite regular.

Histological frontal section of the upper half of the femur (HES staining). e=epiphysis; ol=ossification line; d=diaphysis.

High magnification of the growth plate (HES staining).
The chondro-osseous junction line was clearly drawn with insufficiency and disorganisation of diaphyseal ossification. The trabecular bone had become thin and fan shaped, converging on a fibrous diaphyseal endosteum (fig 6).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
High magnification of the diaphyseal ossification (HES staining).
PAS and alcian blue stains were normally distributed. Myxoid degeneration of cartilage matrix and giant cells were not observed.
Discussion
Our case had clinical characteristics of both AT-I and BD including polyhydramnios, micromelic dwarfism, macrocephaly, micrognathia, depressed nasal bridge, and talipes, but no omphalocele or cleft palate which are more frequent in BD.6 7 Our radiological findings are more in favour of BD: very short, broad, and curved femora, triangular iliac wings, only one ossified long bone, and only the distal phalanges ossified.
This case was a female fetus and all reported cases of BD except one7 have been male. However, only 11 sporadic cases have been reported, which is not sufficient to conclude that BD has X linked recessive inheritance. Our case was also sporadic and could have been caused by a dominant mutation.
Our histopathological findings have never been described either in typical AT-I or in BD. In the two disorders, giant cells, generally in association with hypocellular or acellular areas of cartilage,3 8 9 disorganised growth plate maturation,8-10 and matrix degeneration,10have been described, but in the case reported by Herzberget al 11 as a “variant of atelosteogenesis”, a photomicrograph of the femur of a 20 week fetus showed a short, irregularly shaped bone and probably lateral fan shaped ossification that might be similar to our case. This particular finding was not detailed by the authors. Greally et al,6 in the radiographic study of their case, described the femora as “undertubulated, short and hypoplastic in their distal aspect”. At necropsy, this fan shaped diaphyseal ossification was not mentioned but strongly suggested by the radiographic aspect of one femur.
Thus, the present case does not conform exactly to any previously reported severe lethal chondrodysplasia, but could be a “variant of boomerang dysplasia”. This particular lateral fan shaped ossification is perhaps another important histological feature of the nosological group of AT-I and boomerang dysplasia. It is quite similar to the histology of the femur in transgenic mice with overexpression of PTHrP (parathyroid hormone related peptide) described by Weiret al.12 The discovery of new skeletal morphogenetic genes will help to explain the pathogenesis and classification of these lethal chondrodysplasias.
Acknowledgments
The authors are grateful to the obstetrician Dr J C Danais (Avranches Hospital) for his help.