Article Text

Abstract
Objective: To test the hypothesis that gene–gene interaction of the renin–angiotensin system is associated with an effect on the extent of coronary atherosclerosis.
Setting and results: A cohort of 1162 patients with coronary artery disease were genotyped for genetic polymorphisms in the renin–angiotensin system. Patients carrying the D allele of the angiotensin I converting enzyme (ACE) gene had greater coronary extent scores (defined as the number of coronary segments with 5% to 75% stenosis) than those not carrying this allele (p = 0.006 in non-parametric analysis and p = 0.019 in parametric analysis). This association remained significant after adjusting for age, body mass index, hypertension, and diabetes, which were also significantly associated with coronary extent scores. There was a significant interaction (p = 0.033) between genotypes of ACE and angiotensin II type 1 receptor (AGTR1). The association between the ACE gene D allele and increased coronary extent scores was significant (p = 0.008 in non-parametric and p = 0.027 in parametric analysis) in those carrying the +1166 C allele of the AGTR1 gene, but was absent in those not carrying the AGTR1 gene +1166 C allele.
Conclusion: These findings suggest that variation in the ACE and AGTR1 genes and their interaction may not only contribute to susceptibility of coronary artery disease as previously found but also modify the disease process, thus contributing to interindividual differences in severity of the disease.
- renin
- angiotensin system
- genetic polymorphism
- gene
- gene interaction
- coronary artery disease
- ACE, angiotensin I converting enzyme
- AGT, angiotensinogen
- AGTR1, angiotensin II type 1 receptor
- AGTR2, angiotensin II type 2 receptor
- CAD, coronary artery disease
- D, deletion
- I, insertion
- PCR, polymerase chain reaction
Statistics from Altmetric.com
- ACE, angiotensin I converting enzyme
- AGT, angiotensinogen
- AGTR1, angiotensin II type 1 receptor
- AGTR2, angiotensin II type 2 receptor
- CAD, coronary artery disease
- D, deletion
- I, insertion
- PCR, polymerase chain reaction
The renin–angiotensin system includes a two enzyme cascade where angiotensinogen (AGT) is cleaved by renin to form angiotensin I, which in turn is processed by angiotensin I converting enzyme (ACE) to generate the effector peptide angiotensin II. The effects of angiotensin II are mediated by cell surface receptors, angiotensin II type 1 receptor (AGTR1), and angiotensin II type 2 receptor (AGTR2). In addition to its role in regulating vascular tone and arterial blood pressure, this system is also involved in vascular endothelial dysfunction and apoptosis, lipoprotein peroxidation, proinflammatory cytokine production, vascular smooth muscle cell proliferation, and vascular matrix synthesis, all of which are important mechanisms in the formation and progression of atherosclerosis.1–3
In view of the pathophysiological role of the renin–angiotensin system and the established benefits of ACE inhibitor,4 it has been proposed that genetic variants affecting the function of this system are candidates for genetic factors for cardiovascular disease. A polymorphism resulting from the insertion (I)/deletion (D) of 287 nucleotides in intron 16 of the ACE gene has been extensively studied in relation to risk of myocardial infarction.5–8 It has also been shown that the ACE I/D polymorphism and a polymorphism arising from an A>C substitution at nucleotide position 1166 in the AGTR1 gene exert synergistic effects on risk of myocardial infarction, such that the ACE D/D genotype is associated with increased risk of myocardial infarction only in those carrying the AGTR1 +1166C allele.9
The severity of coronary atherosclerosis positively correlates with levels of AGTR1 expression in coronary arteries.10 In this study, we tested the hypothesis that the above mentioned epistatic interaction between the ACE and AGTR1 genes is also associated with an effect on the extent of coronary atherosclerosis. The ACE gene I/D polymorphism and the AGTR1 gene +1166 A>C polymorphism were analysed in a cohort of 1162 white British patients with angiographically documented coronary artery disease (CAD). In addition, we examined whether the extent of coronary atherosclerosis was associated with variation in the AGT and AGTR2 genes, which are also components of the renin–angiotensin system.
SUBJECTS AND METHODS
Subjects
We studied a cohort of 1162 patients with angiographically documented CAD. All were white and were recruited from consecutive patients undertaking diagnostic and interventional coronary arteriography in the Wessex Cardiothoracic Unit, Southampton General Hospital, from May 1999 to March 2002. The study was approved by the south and west local research ethics committee, and all subjects gave written consent.
We recorded demographic and clinical data including age, sex, weight, height, occupation, smoking habit, and number of cigarettes consumed per day by each smoker, the presence or absence of hyperlipidaemia (defined as cholesterol concentration > 5.2 mmol/l or triglyceride concentration > 3 mmol/l), current medications, particularly the use of lipid lowering drugs, the presence or absence of hypertension (defined as diastolic blood pressure > 95 mm Hg or systolic blood pressure > 160 mm Hg), the presence or absence of type I or type II diabetes, the presence or absence of previous myocardial infarction, and the presence or absence of CAD in first degree relatives under 65 years of age. Total cholesterol and triglyceride concentrations were measured by the clinical chemistry department of the Southampton General Hospital using standard quality controlled enzymatic methods. Table 1 summarises the characteristics of the patients.
Characteristics of patients
Coronary angiograms were analysed by a consultant cardiologist. The extent of CAD was assessed using a scoring system described by Moise and colleagues11,12 and the coronary extent score was defined as the number of coronary segments (15 in total) with 5% to 75% stenosis. This extent score definition is related to a pathophysiological rather than a haemodynamic concept: the minimal and moderate lesions have a high potential for progression, whereas the more severe (> 80%) lesions are more likely subject to thrombotic, occlusive modifications than to a primary atherogenic progression.11,12 This scoring system has been used in a number of other studies.12,13 The reproducibility of this method has been previously assessed, with an overall variability of 14.1%.12,14
Given that the ACE gene D allele and the AGTR1 gene C allele had population frequencies of approximately 0.5 and 0.3, respectively, and on the basis of findings in previous studies that the ACE gene I/D polymorphism was associated with an odds ratio of about 1.2 whereas the AGTR1 gene A+1166C polymorphism per se was not associated with CAD,5–8 this study had 80% power to detect a gene–gene interaction associated with a 10% increase in CAD risk in a two sided analysis at the 0.05 significance level.15,16
Genotype analyses
A 10 ml blood sample was taken from each subject and DNA was extracted using a salt precipitation method.17 Genotypes for the ACE I/D polymorphism were determined with the use of an allele specific polymerase chain reaction (PCR) method described by Evans and colleagues.18 Genotypes for the AGT gene T174M, AGTR1 gene +1166 A>C, and the AGTR2 gene +1291 G>T and +1297 G>A polymorphisms were determined with the use of the tetraprimer amplification refractory mutation system PCR method as described previously.19 Table 2 gives the primer sequences and PCR conditions. Each PCR reaction was performed in a total volume of 10 μl containing 20 ng of template DNA, 1 × PCR buffer (Life Technologies, Paisley, UK), 200 μM deoxynucleotide triphosphate, appropriate concentrations of primers and MgCl2 as described in table 2, 1.5 M Betaine and 0.5 U DNA Taq polymerase. A 5 μl aliquot of PCR product was subjected to microplate array diagonal gel electrophoresis.20 The gel was stained with Vistra green (Amersham Pharmacia Biotech, Little Chalfont, UK) and scanned with a fluorimager 595 (Molecular Dynamics, Sunnyvale, California, USA).
Polymerase chain reaction primers and conditions
Statistical analyses
χ2 analyses were performed to test whether the observed genotype distributions deviated from Hardy-Weinberg equilibrium. The Kruskal-Wallis non-parametric test and analysis of variance were used to examine whether coronary extent scores differed between patients with different genotypes. To test whether the reported epistatic interaction between the ACE gene D allele and the AGTR1 gene +1166C allele was also associated with an effect on the extent of coronary atherosclerosis, we used the same genetic model as previously described9—that is, the relation between coronary extent score and ACE genotype was assessed separately in groups of subjects with different AGT1R genotypes. The analyses were carried out using the SPSS package (version 11, SPSS Inc, Chicago, Illinois, USA).
RESULTS
A cohort of 1162 patients with angiographically documented CAD were genotyped for the ACE gene I/D, AGT gene T174M, AGTR1 gene +1166A>C, and AGTR2 gene +1291G>T and +1297G>A polymorphisms. Table 1 summarises the characteristics of the patients. The genotype frequencies for all polymorphisms were consistent with Hardy-Weinberg equilibrium. The frequencies of the ACE gene D, AGT gene 174M, AGTR1 gene +1166C, AGTR2 gene +1291T, and AGTR2 gene +1297A alleles were 0.55, 0.14, 0.30, 0.25, and 0.50, respectively, similar to findings from other studies of white subjects.21 There was no difference between genotype groups in age, sex, body mass index, plasma cholesterol concentration, plasma triglyceride concentration, hypertension, diabetes, and incidence of myocardial infarction.
A significant association was observed between the ACE gene I/D polymorphism and the extent of coronary atherosclerosis, such that patients carrying the D allele had higher coronary extent scores than those not carrying this allele (p = 0.006 in non-parametric analysis and p = 0.019 in parametric analysis; table 3). The association between the D allele bearing genotypes and greater coronary extent scores remained significant (p = 0.024) after adjusting for other risk factors that were also significantly associated with coronary extent scores, including age, body mass index, hypertension, and diabetes (table 3). No association was detected between coronary extent scores and the other polymorphisms studied, when they were analysed individually.
Effect of genotypes on coronary extent scores
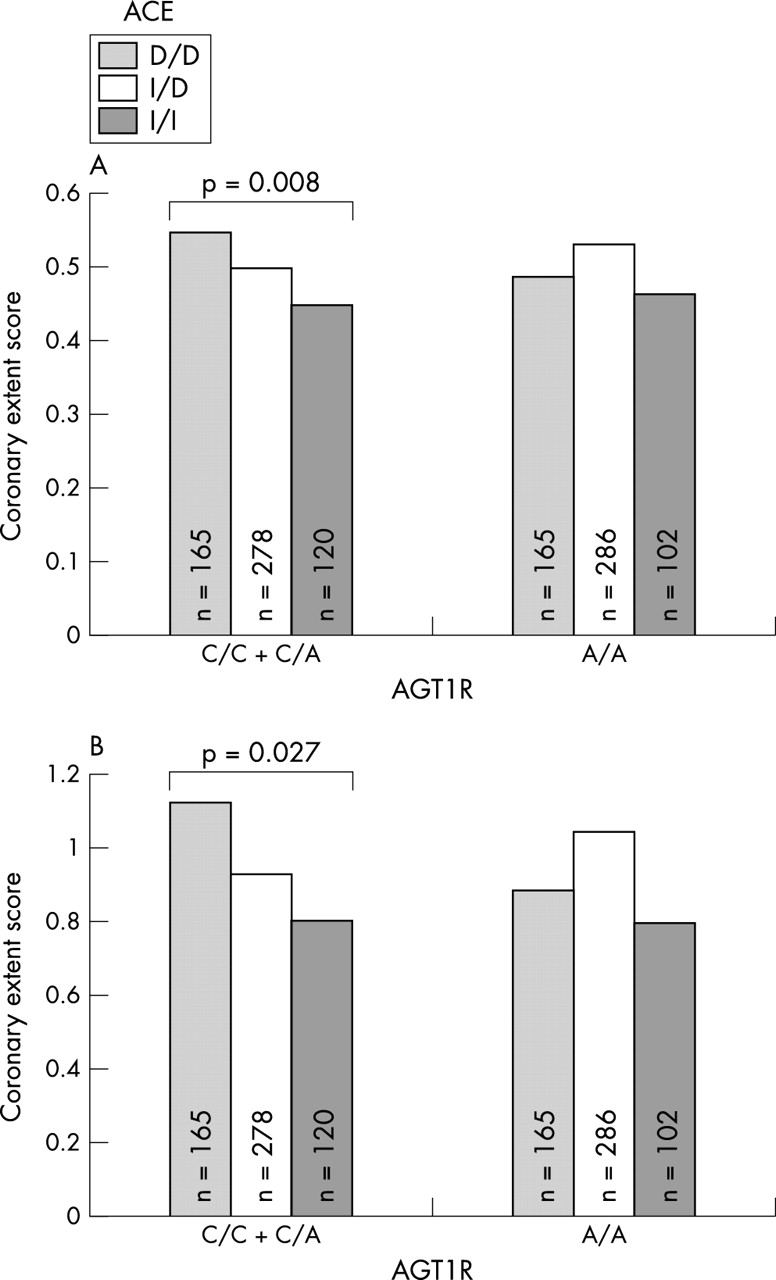
Since an epistatic interaction between the ACE gene I/D and AGTR1 gene +1166 A>C polymorphisms in determining risk of myocardial infarction had been reported, we examined whether this epistatic interaction was also associated with the extent of coronary atherosclerosis, using the same genetic model as previously described.9 Analysis of variance with coronary extent score as the dependent variable showed a significant interaction (p = 0.033) between ACE and AGTR1 genotypes. Further analyses showed that the association between the ACE gene I/D polymorphism and coronary extent scores was highly significant (p = 0.008 in non-parametric analysis and 0.027 in parametric analysis with adjustment for covariates) in patients carrying the C allele of the AGTR1 gene +1166 A>C polymorphism, but was absent in those not carrying the AGTR1 gene C allele (fig 1). There was no interaction between the other polymorphisms studied.

{kind=link}
Bar charts showing an association of angiotensin I converting enzyme (ACE) genotype with coronary extent score only in patients carrying the angiotensin II type 1 receptor gene +1166 C allele. (A) Mean rank in non-parametric test; (B) mean score after adjusting for age, body mass index, hypertension, and diabetes in multivariate analysis of variance. Light grey bars: ACE deletion D/D genotype; open bars: ACE insertion I/D genotype; dark grey bars: ACE I/I genotype.
DISCUSSION
Following the landmark study of Cambien and colleagues,22 which showed an association between the ACE gene I/D polymorphism and risk of myocardial infarction, there has been a large number of studies on this and other genetic variants in the renin–angiotensin system in relation to various cardiovascular disorders. There is now compelling evidence of a strong association between the D allele of the ACE gene and increased plasma ACE concentrations.23 Many studies have also shown that the ACE gene D allele is associated with a modest increase in risk of CAD, myocardial infarction, and ischaemic cerebrovascular disease.5–8 In this study, we tested the hypothesis that genetic variation in this system was also associated with an effect on the extent of coronary atherosclerosis in patients with CAD. A large cohort of patients with angiographically documented CAD was genotyped for polymorphisms in the ACE, AGT, AGTR1, and AGTR2 genes. Extent of coronary atherosclerosis was found to be greater in patients carrying the ACE gene D allele than in those not carrying this allele. In addition, we detected an epistatic interaction between the ACE gene I/D and AGTR1 +1166 A>C polymorphisms, with a synergistic effect of the ACE gene D and AGTR1 gene +1166C alleles on the extent of coronary atherosclerosis.
The data from this study indicate that variation in the ACE and AGTR1 genes may act as genetic modifiers of atherosclerosis. Atherosclerosis is a multifactorial, polygenic disease whose pathogenesis involves gene–gene and gene–environment interactions. The genetic factors may be classified as susceptibility genes and modifier genes; the former contribute to the initiation of the pathogenesis and the latter influence the progression and severity of the disease after it has been initiated.24–26 Identifying the susceptibility genes and modifier genes, as well as their interactions, will help our understanding of the disease mechanisms and may identify targets for developing novel treatment measures.
The I/D polymorphism of the ACE gene arises from the presence or absence of a 287 base pair Alu repeat element in intron 16, and it remains unclear whether this polymorphism itself has a functional effect on the expression or function of ACE or marks the effect of certain functional polymorphism(s) nearby through linkage disequilibrium. Addressing this question would be a challenging task, especially as the I/D polymorphism is in absolute linkage disequilibrium with at least 17 other polymorphic sites at the ACE locus.27 Similarly, it is unknown whether the AGTR1 gene +1166 A>C polymorphism, which is located in the 3′ untranslated region of the gene, has a direct functional effect.
A previous study in white Germans showed that the AGT T174M polymorphism was associated with the extent of coronary atherosclerosis.28 The present study in white British subjects did not detect such an association. The discrepant findings between the two studies may be due to different genetic backgrounds between the two samples or other factors. There has been no reported study on AGTR2 gene variation in relation to coronary atherosclerosis. Although the AGTR2 gene is also a good candidate, particularly as it is located in a region on the X chromosome that has been shown to be in linkage with CAD,29 we did not detect an association between the AGTR2 gene polymorphisms studied and the extent of coronary atherosclerosis.
In summary, this study has identified a synergistic effect of the ACE and AGTR1 genes on the extent of coronary atherosclerosis. The finding suggests that variation in the ACE and AGTR1 genes and their interaction may not only contribute to susceptibility of CAD as previously found9 but also modify the disease process, thus contributing to interindividual differences in severity of the disease.
Acknowledgments
This work was supported by the British Heart Foundation (grants PG/98183). SD was funded by the UK Medical Research Council (G9828424).