Article Text

Abstract
OBJECTIVE Vitamin B12 deficiency is a systemic disease that often affects the nervous system. One of the most prevalent manifestations is subacute combined degeneration (SCD) of the spinal cord. To access the clinical, electrophysiological, and structural abnormalities associated with SCD, a study was conducted in nine patients.
METHODS Clinical, electrophysiological (electroneurography, somatosensory and motor evoked potentials), and MRI evaluations were performed in patients before and after treatment.
RESULTS The most prominent clinical and electrophysiological findings in all patients were dysfunctions of the posterior column. Corresponding hyperintense lesions in the posterior column of the spinal cord were found in two patients by T2 weighted MRI. Damage to the central motor pathway was identified in four patients. Demyelinating neuropathy was present in one patient and axonal neuropathy in four. All patients showed improvement of their symptoms after treatment with cobalamin. Abnormalities of the spinal cord on MRI disappeared early in recovery. Motor evoked potentials and median somatosensory evoked potentials typically normalised after treatment, whereas tibial somatosensory evoked potentials remained abnormal in most patients.
CONCLUSIONS Clinical, electrophysiological, and MRI findings associated with SCD in vitamin B12 deficiency are diverse. Thus vitamin B12 deficiency should be considered in the differential diagnosis of all spinal cord, peripheral nerve, and neuropsychiatric disorders.
- vitamin B12 deficiency
- subacute combined degeneration
- myelopathy
Statistics from Altmetric.com
Vitamin B12 deficiency causes a wide range of haematological, gastrointestinal, psychiatric, and neurological disorders.1 Megaloblastic anaemia is a common early symptom leading to the diagnosis, although neurological symptoms may occur in the absence of haematological abnormalities.2 The neurological syndromes associated with vitamin B12deficiency include myelopathy, neuropathy, neuropsychiatric abnormalities, and less often, optic nerve atrophy. The spinal cord affliction called subacute combined degeneration (SCD) is clinically characterised by symmetric dysaesthesia, disturbance of the position sense, and spastic paraparesis or tetraparesis.1 Although most patients respond well to cobalamin treatment, residual neurological abnormalities persist in most.3 Studies involving limited numbers of patients with cobalamin deficiency have shown various abnormal electrophysiological findings4-9and more recently lesions of the cervical spinal cord by MRI.10-12
Here, we present clinical, electrophysiological, and MRI findings of nine patients affected by SCD. Seven of these patients were followed up after treatment.
Materials and methods
The retrospective study was carried out between 1989 and 1996. Our report includes patients meeting all of the following criteria: low vitamin B12 serum concentrations or abnormal Schilling test, clinical signs of myelopathy, clinical improvement after cobalamin treatment, and no other spinal cord or peripheral nerve disease.
Routine blood chemistry, blood cell, and vitamin B12 serum concentration analyses were performed in all patients. Schilling tests were conducted in four patients.
To define the severity of neurological impairment, we used a previously described functional disability scale3: gait disturbance (=unable to maintain the Romberg position, 2=impairment, but able to walk unsupported, 3=substantial support required for ambulation, 4=wheelchair or bed bound); sensory disturbance (hypaesthesia, dysaesthesia, position sense impairment)(1=impairment only in toes and fingers, 2=in ankle and wrists, 3=in upper arms and legs), and mental impairment(1=intellectual or behavioural impairment but requires no social support, 2=partially dependent for activities of daily living, 3=completely dependent for all activities of daily living). Neuropathy was clinically graded by the loss of reflexes4 (1=loss or reduction of ankle deep tendon reflexes, 2=patellar deep tendon reflexes, 3=deep tendon reflexes of the arms) and severity of pyramidal tract damage was graded as 1=positive Babinski sign, 2=spastic paraparesis, or 3=spastic tetraparesis. The interval between diagnosis and last follow up was 5 to 65 months.
Electroneurographical and EMG studies were performed in all patients, using Amplaid (EMG 15) equipment. Standard techniques were applied to measure nerve conduction13; EMG was performed with standard concentric needle electrodes. Insertion activity, spontaneous activity, and interference pattern were analysed. A minimum of 10 different needle positions at two different sites in each muscle were studied to detect active denervation.
Somatosensory evoked potentials (SEPs) were elicited by unilateral percutaneous stimulation (0.2 ms square wave pulse) at 3 Hz. Stimuli were delivered at an intensity just above motor threshold. Medial SEPs (SEP-Med) were recorded from the brachial plexus (Erb potential), cervical spine at C2 (N13), and the contralateral parietal area 2 cm posterior to C3/4 (N19) with a frontal (Fz) reference. In tibial SEPs (SEP-Tib), active electrodes at the level of the first lumbar vertebra (N22) and at Cz (P37) were referenced to the iliac crest and Fz respectively.
Motor evoked potentials (MEPs) were recorded bilaterally with surface electrodes from the hypothenar muscles and the tibialis anterior muscles. During cortical stimulation a slight voluntary contraction of the target muscles was maintained. The shortest latency evoked by at least four stimuli was analysed. Nerve root stimulation was performed at the C7-Th1 or the L4-L5 level, respectively. Latency differences were used to estimate central motor conduction time.
T1 and T2 weighted, sagittal, and axial MRI images of the spine and skull were obtained with a Siemens Magneton impact (1T)) in five patients, a Phillips gyroscan (1.5 T) in one patient and a Brucker Tomikon (0.23 T) in one patient. When abnormalities were noted, T1 weighted images were retaken after intravenous administration of contrast medium (gadolinium dimeglumine).
Results
PATIENTS’ PROFILE
Six female and three male patients were studied. The underlying diseases causing vitamin B12 deficiency are displayed in table 1. Two patients died of unrelated diseases before the follow up examination. Vitamin B12 deficiency was diagnosed in six patients after admission to our hospital. The remaining patients, diagnosed elsewhere as having haematological disease, developed neurological symptoms as a result of insufficient cobalamin treatment. Laboratory data at the time of clinical presentation are displayed in table 1.
Laboratory and clinical findings
CLINICAL EVALUATIONS
On admission all patients presented gait disturbance, confirmed by the medical examination. Hypaesthesia, dysaesthesia, and impairment of vibration perception or position sense was present in all patients (table 1). Patient H had hyperactive reflexes of the upper limbs. Patellar tendon reflexes were hyperactive in patient A, reduced in patient H, and absent in patient I. In patients A, E, and G ankle reflexes were diminished and in patients H and I they were absent. Toes were upgoing in patients A, C, H, and I with mild paraparesis (patients A, C, and I) or mild tetraparesis (patient H).
Neuropsychological examination disclosed signs of mental impairment with dementia of subcortical type in three patients. Patient C had depression.
After the diagnosis of vitamin B12 deficiency, intramuscular application of cobalmin was started (1000 μg cobalamin once daily for 4 weeks, then once weekly for 1 year followed by long term monthly treatment). All patients reported clinical improvement after treatment. Patient F had completely recovered. The other patients still had gait disturbance, although all patients were able to walk without help. Patients A, C, D, and E complained of sensory disturbance, especially dysaesthesia of the feet. Physical examinations are summarised in table 1.
ELECTROPHYSIOLOGICAL DATA
Electroneurography and electromyography
Neurographical and EMG studies disclosed normal results in patients B, C, F, and G. Patient A showed markedly slowed sensory nerve conduction velocities and normal motor nerve conduction studies (left N. suralis: 26 m/s, 10 μV; left N. peroneus: 41m/s, 4μV; left N. ulnaris (sensible Dig V): 39 m/s, 10 μV; left N. medianus (sensible Dig III): 41 m/s, 20 μV) suggesting a sensory demyelinating neuropathy. Patients D and E had normal motor nerve conduction and only slightly reduced sensory nerve conduction velocities but disproportionally reduced sensory nerve action potentials, suggesting mainly sensory neuropathy of axonal type. Patients H and I showed reduced sensory and motor nerve conduction and EMG signs of acute denervation were present in the extensor digitorum brevis and anterior tibial muscles consistent with a sensorimotor neuropathy of mainly axonal type.
Follow up studies were essentially the same except for patient A, whose sensory nerve conduction velocities of the lower limbs improved from 26 m/s to 36 m/s and normalised at the upper limbs.
Somatosensory evoked potentials
Before initiation of treatment, Tib-SEPs were abnormal in all patients with delayed P37 responses and often absence of the lumbar responses. The Med-SEPs were abnormal in all patients except patients D and F. After treatment SEP-Tibs normalised in patient F. In all other patients the P37 response was still delayed. The SEPs-Med normalised in patients A and C (fig 1 A, table 2).
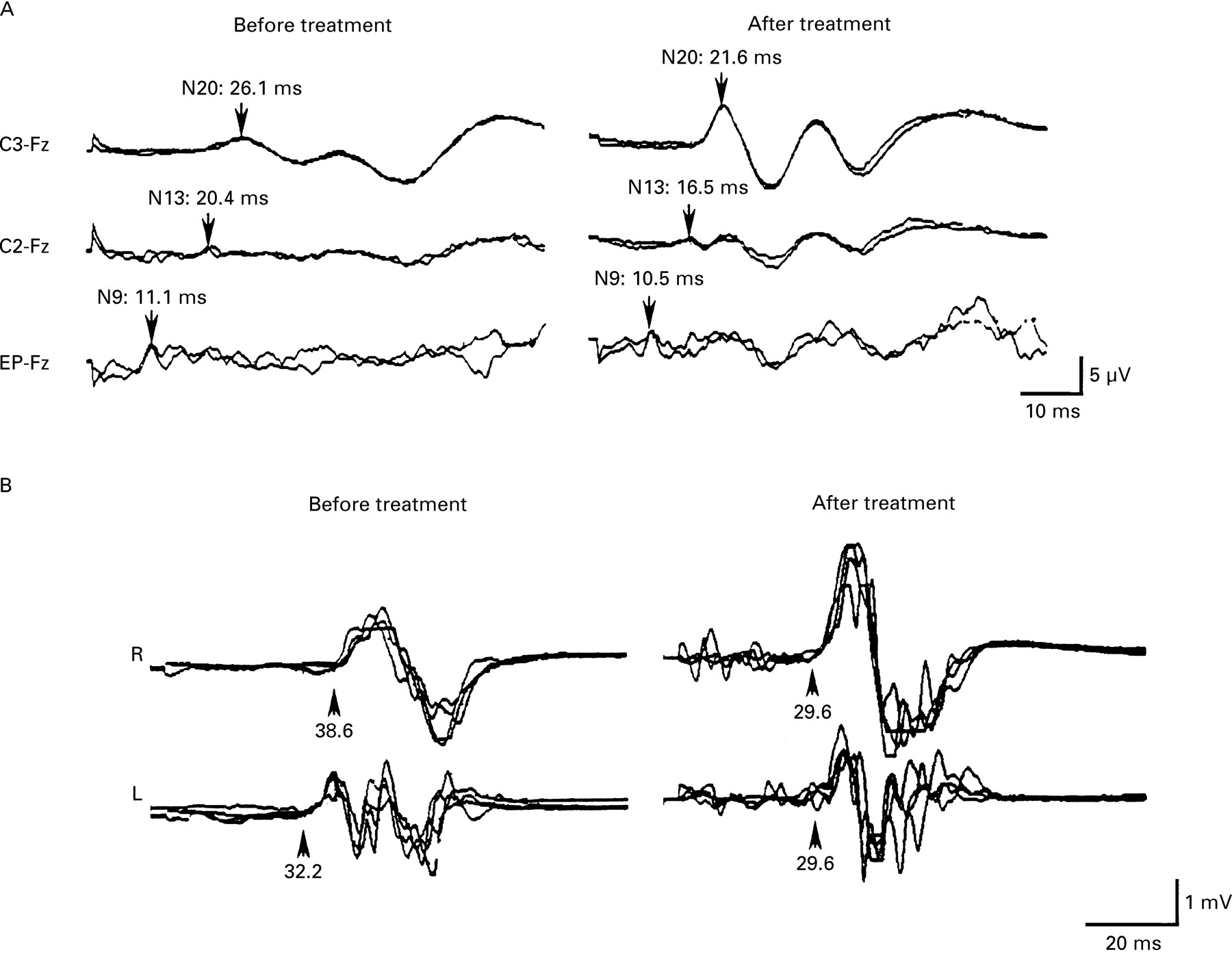
(A) Right median nerve somatosensory evoked potentials of patient A before and after treatment with cobalamin. Recordings were from the contralateral scalp (C3-Fz) neck (C2-Fz)), and Erb’s point (EP-Fz). Note normalisation of N13 and N20 after treatment. (B) Motor evoked potentials of patient C recorded from the right (R) and left (L) anterior tibial muscles after transcranial magnetic stimulation of the motor cortex before and after treatment with cobalamin. Lumbar nerve root stimulation was normal at both examinations. Note normalisation of the corticomuscular latencies after treatment.
Somatosensory evoked potentials in SCD
Motor evoked potentials
Studies of MEPs were performed in seven untreated patients. Before initiation of treatment, patients A, B, D, E, and G had normal central motor conduction times (CMCTs) to the anterior tibial muscles and to the abductor digiti minimi muscles. Patient C showed prolonged CMCTs to both anterior tibial muscles and patient H showed prolongation of the CMCTs to all extremities. After treatment, all patients had normal CMCTs (fig 1 B).
MAGNETIC RESONANCE IMAGING
We performed MRI of the spine in patients A, B, C, and D before and in patients A, B, C, D, E, and F after treatment. Patients A and G underwent MRI of the brain. Before initiation of treatment, patients A and D showed hyperintense lesions within the dorsal columns on T2 weighted images ranging from C2 to C7 (fig 2 1). T1 weighted images were normal and no enhancement was seen after intravenous administration of gadolinium. No abnormalities were found in patient B and C using either high field or low field MRI. All MRI examinations of the spinal cord performed after treatment were normal; MRI of patients A and D (fig 2 2) normalised 8 and 12 months after the initiation of treatment. Patient G had no cerebral abnormalities. Patient A, who was affected by dementia, had diffuse bright lesions around the fourth ventricle on T2 weighted images; no enhancement in T1 weighted images after gadolinium administration was seen. Although the spinal lesions in this patient resolved, the hyperintense lesions of the brain persisted after 8 months.

{kind=link}
{kind=link}
T2 weighted sagittal (A) and axial (B) MRI of the cervical and upper thoracic spinal cord of patient D during initial admission with SCD (1) and 12 months after initiation of cobalamin treatment (2). The hyperintense lesions of the posterior column disappeared after treatment.
Discussion
Since the beginning of this century, SCD has been a well defined disorder with dysaesthesia, disturbance of position sense, and spastic paraparesis or tetraparesis. The corresponding neuropathological findings are a diffuse, multifocal pattern of axonal loss and demyelination most severe in the cervical and thoracic spinal cord. The disease predominantly affects the posterior columns followed by the anterolateral and anterior tracts.14
The pathophysiological mechanism of damage to the nervous system is still not fully understood. Adenosylcobalamin is required as a cofactor for the conversion of methylmalonyl CoA to succinyl CoA. Lack of adenosylcobalamin may lead to accumulation of methylmalonyl CoA, causing a decrease in normal myelin synthesis and leading to incorporation of abnormal fatty acids into neuronal lipids. Alternatively, impaired DNA synthesis could hinder oligodendrocyte growth and thus myelin production.15
The clinical profile of our patients was dominated by damage to the posterior column of the spinal cord. The major findings were dysaesthesia and gait disturbance with impairment of position and vibration sense in the lower limbs and often in the upper limbs. The SEP studies disclosed significantly delayed cortical response in most patients accordingly.5 8 9 Signs of damage to the central motor pathway were present only in four patients, but only two had abnormal MEPs.9 This indicates that damage to the pyramidal tract is less frequent and SCD should also be considered in patients with pure afferent fibre damage. Clinical evidence for peripheral neuropathy was found in five patients. Four of them had axonal neuropathy,4 6 7 but one patient had definite severe sensory demyelinating neuropathy. Neuropsychological manifestations of cobalamin deficiency were seen in three patients.
All patients improved after treatment, but most complained of residual symptoms such as dysaesthesia and gait disturbance. All patients who underwent follow up examination showed residual abnormal findings, mainly impairment of proprioception and mild to moderate dysaesthesia. Two patients still had clinical improvement up to 3 years after onset of cobalamin treatment. Three patients showed little improvement after initial treatment. However, two of them had discontinued the recommended long term treatment schedule. The SEPs-Med normalised after therapy, whereas SEPs-Tib remained abnormal in most patients. Electrophysiological findings in axonal neuropathy were essentially unchanged at follow up examination as reported previously.6 By contrast, demyelinating neuropathy resolved in one patient after treatment. This proves that in rare cases vitamin B12 deficiency may lead to a primarily demyelinating, reversible neuropathy.16
We performed MRI of the spinal cord in four untreated patients and found hyperintense lesions restricted to the posterior column in two of them. Both patients showed clinical and electrophysiological damage to the posterior column and no signs of pyramidal tract involvement. In one patient, MRI of the brain disclosed diffuse hyperintense lesions around the fourth ventricle. After treatment with cobalamin the hyperintense lesions of the spinal cord were resolved after 8 to 12 months. Interestingly no change in the cerebral lesions was found. Corroborating findings by other investigators10-12 as well as ours indicate that hyperintense T2 lesions of the posterior column may be common in SCD, but are not present in every patient. We found no strict correlation between clinical, electrophysiological, and MRI abnormalities in our patients.
In summary, subacute combined degeneration is clinically characterised by predominant affection of the posterior column resulting in impairment of position and vibration sense and dysaesthesia. In some patients, MRI shows abnormalities of the spinal cord, indicating demyelination of the posterior column. Involvement of the pyramidal tract and peripheral neuropathy are less pronounced or may be absent. If neuropathy is present, it is mostly axonal and sensory. In rare cases, vitamin B12 deficiency can induce demyelinating neuropathy. Normal tibial nerve SEPs strongly argue against the diagnosis of subacute combined degeneration. In general, SCD responds well to adequate treatment. However, full recovery is exceptional and tibial nerve somatosensory evoked potentials usually remain abnormal even after long term treatment.
Acknowledgments
We thank A Tzou, B Bielekova, and B Gran, Neuroimmunology Branch, NIH for helpful comments on the manuscript.