





Abstract
Mannose-binding lectin has recently been identified as a modifier of severity in cystic fibrosis, although studies have produced differing results and the mechanism of action remains unclear.
The current authors have studied large cohorts of adults (n=298) and children (n=260) to explore this apparent relationship further.
Adults with two structural mutations, but not heterozygotes, had significantly reduced lung function and oxygen saturations, more frequent hospital admissions and raised systemic inflammatory markers. This was not related to increased rates of infection with Pseudomonas aeruginosa, and there was no increased susceptibility to Burkholderia cepacia. None of these findings was mirrored in the paediatric cohort.
In conclusion, severe mannose-binding lectin deficiency appears to be detrimental to cystic fibrosis adults, although heterozygotes are not affected. It is suggested that this is not related to impaired complement-mediated bacterial killing, and a link with the host inflammatory response is hypothesised. If mannose-binding lectin replacement is developed as a new approach to treatment for this disease, the present study would suggest that the small group of severely deficient patients with two structural mutations may be the group to benefit.
This work was supported by the Cystic Fibrosis Research Trust, by a Wellcome Trust Senior Clinical Fellowship (E.W.F.W. Alton), and a Wellcome Trust Clinical Fellowship (K. Fidler). Research at the Institute of Child Health and Great Ormond Street for Children National Health Service (NHS) Trust benefits from research and development funding received from the UK NHS executive. Consumables for this study were funded in part by NatImmune A/S, Copenhagen, Denmark. M.W. Turner and N. Klein are consultants for this company, which is developing a recombinant form of mannose-binding lectin.
Most of the morbidity and mortality in cystic fibrosis (CF) relates to lung disease, characterised by chronic bacterial infection and a sustained and deleterious inflammatory response 1. However, disease severity is highly variable, even in subjects with identical cystic fibrosis transmembrane regulator (CFTR) gene mutations, leading investigators to search for modifier genes, such as alternative ion channels orproteins involved in host defence and inflammation. A collectin, mannose-binding lectin (MBL), has recently been identified as one such modifier 2. Together with the mucociliary escalator, professional phagocytes and other proteins (lysozyme, lactoferrin, defensins, complement), collectins form the first line of airway defence, before the adaptive immune systems come into play. In its functional oligomeric form, MBL binds to carbohydrate arrays on the surface of microorganisms, initiating complement-mediated lysis and acting as an opsonin to facilitate phagocyte function 4. The protein also influences the inflammatory response in a complex and incompletely understood manner 5.
Three polymorphisms have been identified within the structural region of the encoding gene, MBL-2 6. Mutant proteins are incapable of forming high-order oligomers and possess shortened half-lives. Individuals with two mutations have profoundly reduced levels of MBL, whilst intermediate levels are observed in heterozygotes. Polymorphisms have also been identified within the promoter region of MBL-2, in linkage disequilibrium with the structural mutations, and one of these (X/Y) significantly affects protein levels 8. As heterozygotes comprise >30% of the healthy population, MBL is likely, in general, to play only an adjunctive role in host defence. However, low protein levels relate to an increased risk of a variety of infections 9–11, including those of the respiratory tract 12. The detection of MBL in human nasopharyngeal secretions 13 provides further evidence for a role of the protein in respiratory defence.
Two previous studies reported that MBL-2 was a modifier of lung disease in CF, although these reports conflicted on whether the effect was limited to the homozygous-deficient state seen in only 3–4% of individuals 3 or whether it was also seen in the 30% of the population carrying a single mutation 2. This differentiation would have important implications for the development of MBL replacement as a treatment for CF. In an attempt to explore this further, the current authors have correlated MBL-2 haplotype status with clinical markers of severity in a large cohort of both adults and children with CF.
Methodology
Patients and clinical data
Patients were recruited from the adult and paediatric CF clinics at the Royal Brompton Hospital, London, UK, between 2000 and 2002. Samples were obtained at the time of a routine blood test whenever possible. Clinical data were obtained from the clinical databases, patients' hospital notes and computerised microbiology reports. Forced expiratory volume in one second (FEV1) and forced vital capacity (FVC) were obtained from annual lung function laboratory records, corrected for sex, age and height, and expressed as a percentage of predicted normal values 14. For the paediatric cohort, lung function was recorded for specific ages for purposes of standardisation (6–7, 8–9, 10–11, 12–13 and 14–16 yrs). For adults, annual values were recorded, where available, from 1990–2002. Annual rate of decline was calculated for all subjects with two or more values after linear regression of all available data. For the adult patients, transcutaneous oxygen saturation with the patient breathing room air was obtained at the annual visit, and a record of therequirement for supplementary oxygen was made. Microbiological data included the presence of any samples positive for Psuedomonas aeruginosa and Burkholderia cepacia.In the paediatric group only, data were also available for Stenotrophomonas maltophilia, Staphylococcus aureus and Aspergillus fumigatus. C-reactive protein (CRP) and white cellcounts were reported by the clinical biochemistry and haematology laboratories of the Royal Brompton Hospital, respectively. A further 38 blood samples were analysed from B. cepacia-infected patients from three other UK CF centres. No further clinical data were obtained on these subjects.
Clinical parameters were compared between three MBL-2 haplotype groups (wild-type homozygous, heterozygous and homozygous/compound heterozygous deficient). Subsequently, each adult patient with two copies of the mutant allele was retrospectively matched with two adults with no MBL-2 mutations for further comparison. Matching was performed on the basis of age (closest within 5 yrs), sex and CFTR genotype (Δ/Δ, Δ/other or other/other). If more than two matches were available, the patient was paired with the nearest two subjects in a randomly generated list.
The study was approved by the ethics committees of the Royal Brompton Hospital, Harefield Hospital, and the National Heart and Lung Institute and participating centres, and all subjects, parents or carers gave informed consent for participation.
Sample analysis
Preparation and amplification of genomic DNA and MBL-2 haplotyping were performed as previously described 15. Genotyping was performed separately for the exon-1 mutations and the promoter polymorphisms. In both cases, a synthetic DNA molecule (universal heteroduplex generator (UHG)) was constructed, spanning the region of interest and containing insertions, deletions and/or substitutions. The combined use of these UHGs (kindly provided by N. Wood, University of Bristol, Bristol, UK) permitted the detection of all possible known mutations. MBL levels in serum were determined by a symmetrical sandwich ELISA, using a kit from the State Serum Institute, Copenhagen, Denmark, according to the manufacturer's instructions.
Statistical analysis
Differences between haplotype groups were analysed by one-way ANOVA with Tukey's post hoc comparisons or by Chi-squared analysis. Fisher's exact test was used for groups containing fewer than five values. Data are presented as mean±sem. The null hypothesis was rejected at p<0.05.
Results
Patient demographics
Blood samples were available from 298 (57% male) adult subjects aged 29.7±0.5 yrs. CFTR genotype data were available on 269 (90.3%) of these, as follows: Δ/Δ (48%), Δ/other (44.6%), and other/other (7.4%). A total of 260 children (48% male) with a mean age of 8.5±0.3 yrs were included. In 228 children, CFTR genotype data were available, as follows: Δ/Δ (58.8%), Δ/other (34.6%) and other/other (6.6%).
Mannose-binding lectin-2 haplotypes and serum levels
Both MBL serum levels and MBL-2 haplotype data were available in 522 cases; in 7 cases, only haplotypes were obtained and, in 25, only protein levels were available. The frequencies of mutations in both exon 1 (fig. 1a⇓) and the promoter region did not differ between adults and children, and were similar to those observed in other studies of both healthy subjects 17 and patients with CF 2. Overall, 61.1% had no structural mutations (conventionally designated A/A), 35.2% were heterozygous (designated A/O) and 3.8% were either homozygous or compound heterozygous (both designated O/O). In patients with structural gene mutations, the B allele was found on 71% of chromosomes, with the other mutations occurring less frequently (C: 11%, D: 18%). The low-expressing X-promoter polymorphism was found in association with 30.6% of wild-type structural alleles.

a) The frequency of mannose-binding lectin (MBL)-2 gene structural mutations was similar amongst the adult (└) and paediatric (□) cohorts. A represents the wild-type allele and O any mutation (B, C, or D). b) MBL serum level was significantly related to MBL-2 haplotype (p<0.001). Serum levels in each haplotype group were similar in the adult and paediatric groups, with the exception of the YA/YA group, in which levels were significantly higher in the adults. Data are presented as mean±sem. ***: p<0.001.
Serum MBL level was significantly related to MBL-2 haplotype (fig. 1b⇑; p<0.001). The highest protein levels were seen in patients with two wild-type structural alleles, and the lowest in individuals with two structural mutations and in heterozygotes with the X-promoter mutation. Levels were similar in adults and children, with the exception that adults with the YA/YA haplotype had significantly (p<0.001) higher levels (3858±221 ng·mL−1) than those observed in the paediatric cohort (2959±139 ng·mL−1). As a result, the adult homozygous-sufficient A/A subjects had significantly (p<0.05) higher levels than the A/A children.
Lung function, infection and inflammatory markers
Different results were observed with respect to the adults and paediatric subjects, and these groups are therefore presented separately.
Adults
Lung function
A mean of 6.1±0.2 lung function recordings (range 1–13) was available on 273 haplotyped adults over a period of 6.5±0.2 yrs. Mean FEV1 was significantly associated with MBL-2 haplotype, the lowest values being observed in individuals possessing two structural mutations (fig. 2a⇓; ANOVA p<0.05). A similar pattern was seen for mean FVC (fig. 2a⇓). Neither parameter was reduced significantly in heterozygotes. No effect was seen of the low-expressing X-promoter polymorphism on lung function in either the homozygous-sufficient or heterozygous groups (table 1⇓). Over the 12-yr time period studied, subjects with the O/O haplotype also had the fastest annual rate of decline in FEV1 (2.2±0.5% of baseline versus 1.3±0.1% in the A/A group and 0.7±0.1% in the A/O group, p<0.001; fig. 2b⇓). Oxygen saturations were significantly (p<0.001) lower in this group (93.2±2.1%) than in either heterozygotes (96.0±0.2%) or wild-type homozygotes (96.0±0.2%; fig. 2c⇓). This was reflected in the requirement for supplementary oxygen, which was highest in the O/O group (O/O 20%; A/A 3.7%; A/O 1.1%; Fisher's exact test p<0.01).
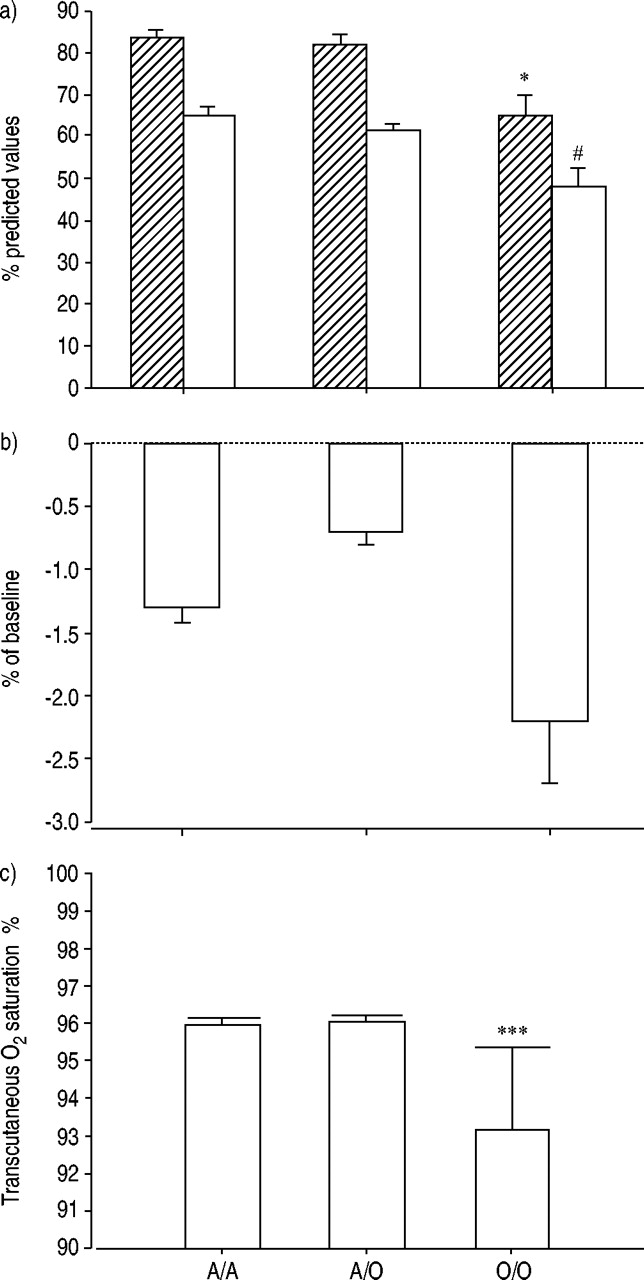
a) In adults, both forced expiratory volume in one second (FEV1; □) and forced vital capacity (└) were significantly different across the three mannose-binding lectin (MBL)-2 haplotype groups (A/A: n=163; A/O: n=99; O/O: n=11; ANOVA p<0.05). The lowest values were seen in subjects with the O/O haplotype (*: p<0.05 versus both other groups; #: p<0.05 versus A/A subjects). The values in heterozygotes were not significantly different from those of wild-type patients. b) Annual rate of decline in FEV1 was calculated on all adult patients with at least two lung function recordings a year apart. Linear regression was performed where three or more recordings were available and the data are expressed as % decline from baseline values. Rates differed significantly across MBL groups (p<0.001), with those possessing two mutations demonstrating the fastest decline (A/A: n=144; A/O: n=85; O/O: n=11). c) Patients possessing two mutant MBL-2 alleles (O/O) had significantly reduced transcutaneous oxygen saturations (***: p<0.001 versus both other groups; A/A: n=145; A/O: n=89; O/O: n=10).
Effect of the X-promoter polymorphism on mean lung function values in either homozygous or heterozygous adults
Infection and inflammation
The majority of the adult cohort (86.7%) had experienced repeated positive cultures for P. aeruginosa, but no significant link was observed with MBL-2 haplotype; as a result of limited numbers of noninfected individuals, further analysis of this effect on the basis of MBL status was not attempted. A total of 18 of the adults were infected at the time of recruitment with B. cepacia and a further 38 patients were recruited from other UK centres. No significant effect of MBL-2 was observed (infected: A/A 57.1%, A/O 39.3%, O/O 3.6%; noninfected: A/A 60.0%, A/O 36.1%, O/O 3.9%; p=0.8). In total, 40.1% of patients had required at least one admission for i.v. antibiotics in 2002; O/O patients had received the greatest number of i.v. courses (fig. 3a⇓; p=0.015). Most recent CRP (obtained at annual assessment) was significantly raised in this group (fig. 3b⇓; p<0.05), with a similar trend in total circulating leukocyte count (fig. 3c⇓; p=0.06).
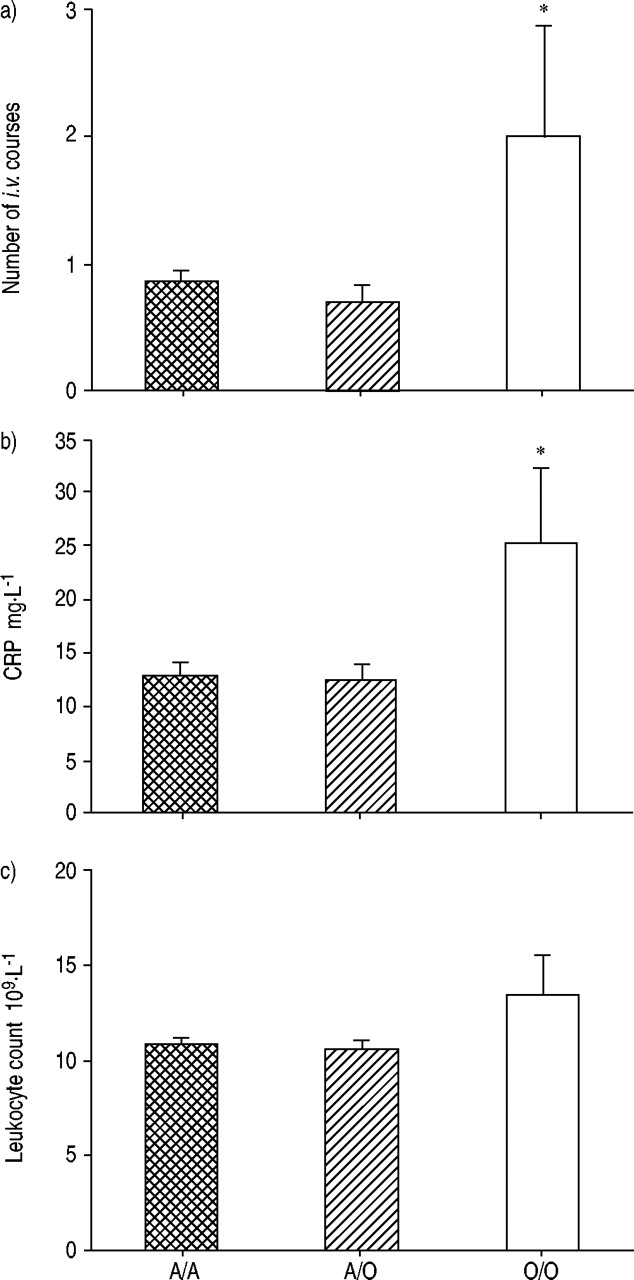
a) Mean number of i.v. antibiotic courses in 2002 differed across mannose-binding lectin-2 haplotypes, with the greatest number being received by O/O adults (*: p<0.05 compared with both other groups; A/A: n=166; A/O: n=103; O/O: n=10). b) O/O adult patients had significantly raised C-reactive proteins (CRPs; *: p<0.05 compared with both other groups; A/A: n=166; A/O: n=103; O/O: n=11). c) A similar trend was seen with regard to peripheral leukocyte count (ANOVA p=0.06; A/A: n=159; A/O: n=100; O/O: n=11).
The clinical disadvantage in the O/O group could not be explained by these patients being either significantly older than the other haplotype groups (A/A: 29.3±0.7 yrs, A/O: 30.4±0.8 yrs, O/O: 31.4±3.4 yrs; ANOVA p=0.5) or by there being an over-representation of patients possessing the Δ/Δ CFTR mutation amongst this group (A/A: 50.7%, A/O: 43.3%, O/O: 55.6%; Fisher's exact test p=0.7). However, to confirm the findings, the data from the 11 O/O subjects was compared with that of A/A controls matched for age, sex and CFTR genotype (table 2⇓). Two A/A subjects were sought foreach O/O individual; however, in one case of a patient aged>50 yrs, only a single sufficiently close match was available. O/O subjects had significantly lower mean lung function values than their matched A/A counterparts (FEV1: 47.6±4.8% versus 66.1±5.7%, p=0.02; FVC: 64.8±4.7% versus 84.7±3.4%, p<0.01) and significantly higher CRP levels (25.3±7.2 mg·L−1 versus 10.7±1.9 mg·L−1, p<0.02).
Comparison between A/A and O/O subjects matched for sex, age and cystic fibrosis transmembrane regulator (CFTR) genotype
Relationship with mannose-binding lectin serum concentration
Despite the close relationship between MBL-2 haplotype and MBL protein levels, there was no direct inverse correlation between the latter and lung function (p=0.17). To explore this discrepancy, lung function was compared between groups divided on the basis of MBL serum level into upper, middle and lower quintiles, where a significant pattern emerged (p<0.05; fig. 4⇓). The highest FEV1 and FVC values were observed in the middle quintile group, with both upper and lower quintile groups demonstrating reduced lung function.

To examine the relationship between mannose-binding lectin levels and lung function, adult patients were divided into groups based on upper ( ), middle (└) and lower (□) quintiles for serum level. Significant differences were seen for both forced expiratory volume in one second (FEV1; p<0.05) and forced vital capacity (FVC; p=0.02), with the highest lung function observed in patients in the middle quintile group.
), middle (└) and lower (□) quintiles for serum level. Significant differences were seen for both forced expiratory volume in one second (FEV1; p<0.05) and forced vital capacity (FVC; p=0.02), with the highest lung function observed in patients in the middle quintile group.
Paediatrics
Lung function
A total of 191 children had their lung function measured on at least one occasion, with the others being too young to perform the manoeuvre. As none of the O/O children was >12 yrs old, all comparisons were made for lung function obtained between the ages 7–11 yrs (mean age A/A: 9.7±0.2 yrs, A/O: 9.7±0.2 yrs, O/O: 8.6±1.0 yrs; ANOVA p=0.3). Neither mean FEV1 nor FVC was reduced at this stage in children possessing the O/O haplotype (fig. 5⇓), and there was no effect of the X-promoter polymorphism (data not shown).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
No significant effect of mannose-binding lectin-2 genotype was seen on forced expiratory volume in one second (□) and forced vital capacity (└) between the ages 7–11 yrs (all recordings were presented as means for each individual). A/A: n=113; A/O: n=67; O/O: n=6.
Infection and inflammation
In total, 85.1% of children had experienced at least one positive culture for P. aeruginosa, and, in 28.8%, the organism had a mucoid phenotype suggestive of chronic infection. For the group as a whole, infection with P. aeruginosa before the first lung function measurement had a significant adverse effect on both FEV1 (87.2±1.7% versus 96.1±2.2%; p<0.01) and FVC (95.2±1.4% versus 101.3±2.1%; p=0.02). However, there was no association between infection rates, age or mucoid conversion and MBL-2 haplotype. By the end of the study, seven children had experienced at least one positive culture for B. cepacia. There was no apparent trend with regard to MBL haplotype (YA/YA: n=3, YA/XA: n=2, YA/O: n=1 and XA/O: n=1). No differences were observed between MBL-2 haplotype groups with regard to ever having been admitted for i.v. antibiotics or age at first admission (data not shown). Neither current CRP nor white blood cell count was significantly different across the three groups (data not shown).
Discussion
In the largest group of CF patients studied to date, the current authors report that adults possessing two abnormal structural MBL-2 alleles have significantly reduced lung function, lower oxygen saturations and an increased requirementfor hospital admission. This may relate to increased levels of inflammation, as CRP was raised, but appears not to be as a result of chronic bacterial infection. These associations were not seen during childhood, which may raise issues relating to the sequence of progression of CF lung disease or to the timing of modifier-gene studies.
Two previous studies have examined the effect of MBL status on lung function in CF 2. As in these studies, the MBL-deficient O/O group in the present study is small, but similar findings in each of the studies lend strength to the conclusions. Gabolde et al. 3 matched 11 MBL-deficient adults (O/O) with homozygous sufficient controls (A/A), and reported that MBL deficiency led to significantly worse lung function. No disadvantage was seen in heterozygotes. In contrast, Grred et al. 2 reported that either one or two structural MBL-2 gene mutations (A/O or O/O) led to the impairment of FEV1 and reduced survival. The current lung function findings concur with the study by Gabolde et al. 3, as it is clearly shown in this large group of adults that structural heterozygotes have normal lung function. This is despite the current observation that a number of the heterozygotes have MBL protein levels within the range seen in patients with two variant alleles.
Wild-type MBL is polymeric in nature with 4–6 subunits, each based on three identical peptide chains associated through a collagenous triple helix. MBL-2 structural gene mutations impair this polymerisation, so that patients possessing two mutated structural alleles do not possess this form of the protein 17. However, in individuals with apparently low or absent levels of wild-type MBL, a low molecular weight monomeric form can exist 18, and may circulate at high levels in some individuals 19. This monomeric form of MBL is not usually detected by commonly used assays, such as that utilised in the present study 20. Whilst the functionality of this form of MBL is unknown, the current results indicate that either small quantities of wild-type MBL, which may be seen in XA/YO individuals, or high levels of monomeric MBL, which may be seen in YO/YO individuals, may be critical in determining the lung function of patients with CF.
How MBL is operating in CF is still unclear. In contrast to Gabolde et al. 3, the current authors are in agreement with Garred et al. 2 that MBL does not influence susceptibility to P. aeruginosa or B. cepacia. This is despite results from the current authors' earlier in vitro study demonstrating high levels of MBL binding to clinical isolates of B. cepacia and subsequent activation of complement 21. Taken together, these findings might suggest that complement-mediated clearance of bacteria is not an important mechanism of action for MBL in the CF lung. Nevertheless, levels of binding that are insufficient to activate complement-mediated bacterial killing may be sufficient to modulate the host inflammatory response to a microbial insult, and the present study provides some clinical evidence to suggest that this may be the case in CF. MBL plays a complex and incompletely understood role in the inflammatory response 5. Low circulating protein levels have been found to be both advantageous and detrimental in different disease settings 22, and a biphasic dose response has been demonstrated in vitro 5. It would appear from the current data that MBL, which is present in the airway surface fluid (ASF), may be exerting an anti-inflammatory action. In addition to the much lower levels of circulating protein available to reach the airways in O/O individuals, recent data suggest that the mutant forms of the protein may be more susceptible to degradation by matrix metalloproteinases that are present in abundance in the CF ASF 24, and, thus, MBL-deficient individuals may be doubly compromised. The current authors are examining this hypothesis further by measuring levels of MBL and inflammatory cytokines directly in CF bronchoalveolar lavage samples.
Two important issues relating to the study of modifier genes in CF have been raised by the present study. The first concerns the apparently different results obtained from our paediatric and adult cohorts. It is recognised that the group of O/O children was very small (n=6), and, thus, this study may have been underpowered to detect a difference in children. This is a recurring problem in modifier-gene studies attempting to examine the effect of fairly rare genotypes. No trends were visible, but the current authors have begun the collection of samples from another paediatric cohort in order to increase numbers. In addition, whilst it is possible that there may be disease stage-specific effects of modifier genes, it is equally likely that any effects are more difficult to detect in the younger age group. Whilst Garred et al. 2 observed an MBL effect in individuals as young as 8 yrs old, most of the children in this study had well-preserved lung function, and low or undetectable levels of systemic inflammatory markers. Thus, with the clinical markers used in this study, any potential modifier gene must exert a very significant detrimental effect before that effect will be apparent, even in a relatively large cohort, such as that of the current authors. This may be become increasingly difficult, as children and adults with CF have significantly better health status than was usual in previous decades 25. Future modifier-gene studies should possibly be conducted initially in adults, in whom the greater variability in severity might facilitate the identification of groups at risk. Alternatively, more sensitive clinical markers, such as, in this case, direct measures of airway inflammation, may be more useful. The second important point relates to the ability to differentiate cause from effect when conducting studies on proteins involved in inflammation or acute-phase response processes. Patients with the lowest serum MBL levels had low lung function. However, patients with the highest levels also had lower lung function than those with intermediate levels. It is hypothesised that, whilst the former group were demonstrating poor lung function as a result of MBL deficiency, the latter group had high protein levels in response to their poorpulmonary status. This hypothesis is supported by thefinding that wild-type (homozygous sufficient) adults hadsignificantly higher MBL levels than the corresponding group of children. This is likely to be the group with the greatest capacity for increasing protein levels in response to stimuli, and the higher levels are likely to reflect the more advanced disease status with increasing age. Follow-up studies in the younger patients may help to confirm this hypothesis. It is suggested that grouping on the basis of nonvariable parameters, such as genotype rather than variable protein levels, may be more likely to yield clear, interpretable results.
In addition to the increased understanding they provide of disease pathogenesis, modifier-gene studies are being conducted with a view to the development of novel forms of therapy. Purified serum-derived mannose-binding lectin has already been administered to patients, including one with cystic fibrosis who appeared to benefit 26. With the advances in recombinant protein technology, mannose-binding lectin may become a treatment option for deficient patients suffering from a variety of diseases. Whilst the current data indicated that the detrimental effect in this disease is limited to those patients with two abnormal copies of the mannose-binding lectin-2 gene (3–4% of cystic fibrosis patients), further studies are required to examine the potential role of mannose-binding lectin therapy in cystic fibrosis.
Acknowledgments
The authors would like toacknowledge the patients and parents for consenting to the study; M. Hodson for allowing access to the clinical database; S. Elborn, S. Conway and D. Bilton for providing samples from B. cepacia-infected adult patients; M. Festing for statistical advice; J. Francis and colleagues in the Paediatric CF clinic for administrative assistance; and L. Somerton, S. Escudera Garcia and the staff of the Clinical Microbiology Laboratory at the Royal Brompton Hospital, London, UK, for technical support.
- Received May 10, 2004.
- Accepted July 15, 2004.
- © ERS Journals Ltd
References









