Article Text

Abstract
Although there are several reports on infant and childhood growth in patients with Sotos syndrome, there is little information on the final height achieved and puberty. Growth data on 40 patients (20 female and 20 male) aged 2–31 years were collected. These showed that patients with Sotos syndrome are excessively tall at birth, during infancy, and during childhood. Disproportionately long limbs constitute much of the increase in stature. However, the combination of advanced bone age and early onset of menarche led to a mean (SD) final height of 172.9 (5.7) cm in women. This is within the normal range for the population. Most of the men also attained a final height (mean, 184.3 cm; SD, 6.0) within the normal range, although exceptions were more likely in men than in women. Therefore, these results show that most patients with Sotos syndrome do not require intervention to limit their adult height.
- Sotos syndrome
- height
- puberty
Statistics from Altmetric.com
The clinical features of Sotos syndrome, first described in 1964, include large body size with early accelerated growth, advanced bone age, acromegaloid features, and developmental delay, with a non-progressive neurological disorder.1 The reported IQ of these individuals ranges from 18 to 119.2
The typical facies include frontal bossing, large head circumference (parallel but above the 97th centile), antimongoloid slant of palpebral fissures, and a prominent jaw. The hands and feet are also large. The syndrome is sporadic in most cases, although some convincing familial cases segregating with an autosomal dominant pattern have been described.3 Diagnosis is based on the recognition of the typical facial gestalt together with the additional features documented above.3 ,4
In infancy, the mean growth rate of children with Sotos syndrome is significantly increased compared with controls.5 However, in childhood, the height velocity becomes similar to that of controls. This growth pattern leads to height that is consistently above the 97th centile in childhood. In many instances, this leads to anxiety that gigantic adult height may be attained.
In our study, we have documented the growth pattern, adult height, (together with the span and upper to lower segment ratio where possible), and age of puberty in individuals with Sotos syndrome.
Patients and methods
Our study had ethics committee approval, and consent was obtained from parents and, where relevant, from the individuals themselves. One of the authors (TC) examined all of the patients to provide consistent confirmation of the diagnosis of Sotos syndrome.
We measured the patient’s height and weight, as well as parent heights, at this visit.
In 24 patients, we measured the arm span, as well as the body segment ratios. We measured the arm span (distance between the finger tips of middle fingers of each hand when the arms are stretched out horizontally from the body) using a tape measure. We also measured the lower body segment (distance from the top of the middle part of the pubic bone to the sole of the feet) using a tape measure. We calculated the upper to lower body segment ratios using the following equation:
 Methods for measuring armspan and body segment ratios as well as standards for normal children have been published previously.6
Methods for measuring armspan and body segment ratios as well as standards for normal children have been published previously.6
Subsequently, we obtained other growth data with the help of individual paediatricians and general practitioners.
We obtained the age of menarche in girls by history from parents and from the case records where possible. Two of the authors (SC and JA) assessed all the bone ages individually (using the Tanner Whitehouse 2 (TW2) method),7 with good agreement between them.
We calculated the mean birth length and the mean height standard deviation scores in the 2nd and 6th years of life. The mean final height is expressed in cm and as mean standard deviation score. We calculated the target height, estimated from parental heights, for those who have attained final height.8 The standard deviation for each calculation is shown.
All patients who received hormonal treatment to limit their adult height were excluded from the final height data.
Results
FACIES
The typical long thin adult facies of patients with Sotos syndrome are shown in fig 1.
Typical facies of children with Sotos treatment. (All photographs reproduced with the permission of the patients.)
GROWTH
Growth data on 40 patients (20 female and 20 male) aged 2 to 31 years were collected and are summarised in table 1. Two women and one man were excluded from the final height data as they had received hormonal treatment to limit their final height.
Growth analysis in patients with Sotos syndrome
The mean (SD) birth lengths of the boys and girls were 55.6 (2.8) cm and 57.3 (3.5) cm, respectively. In boys, the mean (SD) height standard deviation scores in the 2nd and 6th years were 3.58 (1.2) and 3.0 (0.084), respectively. The mean (SD) height standard deviation scores for girls in the 2nd and 6th years were 3.6 (0.08) and 3.8 (1.1), respectively.
The mean (SD) height standard deviation scores achieved at attainment of final height were only 1.51 (0.08) for the men and 1.8 (0.17) for the women. The final height and target height were available for only nine men. The mean target height in these cases was 173 cm compared with the population mean of 175.5 cm, whereas in women the target height was 3.2 cm above the population mean (166.7 cmv 163.5 cm). However, the final height in the men was an average of 11.3 cm greater than the target height compared with only 6.2 cm in the women (table 1).
UPPER TO LOWER SEGMENT BODY RATIO AND SPAN
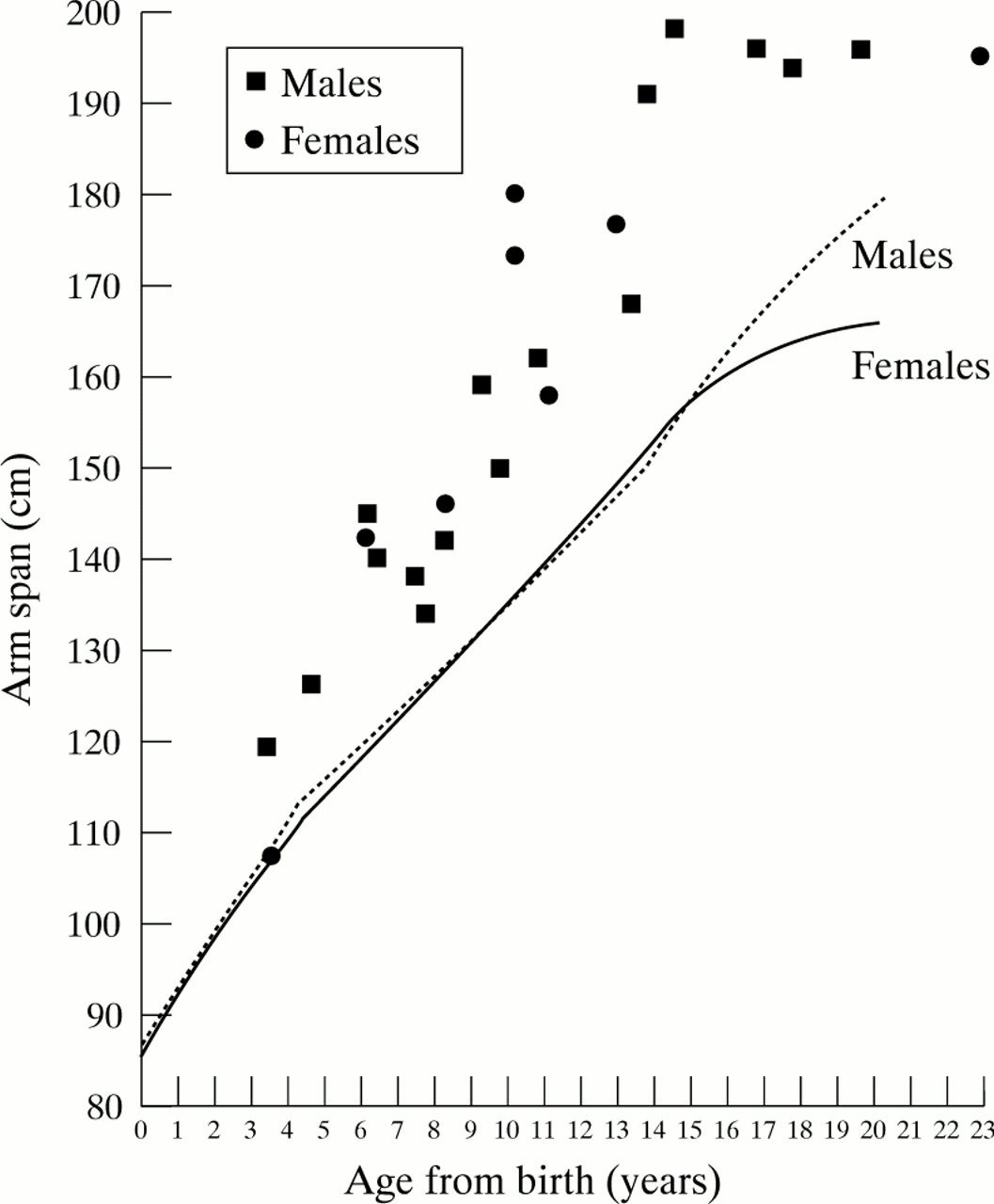
The span and upper to lower segment ratio are plotted on charts indicating normal values for age and sex (figs 2 and 3).6The upper to lower segment ratio was reduced in patients with Sotos syndrome whereas the arm span was increased.

Arm span of patients with Sotos syndrome compared with normal values for age and sex.

{kind=link}
{kind=link}
{kind=link}
Upper to lower body segment ratio in patients with Sotos syndrome compared with normal values for age and sex.
BONE AGE IN SOTOS SYNDROME
Twenty seven x rays (from 13 patients) were available for rating. Bone age was advanced in all patients. In about three quarters of the patients it was advanced more than the 97th centile for age.
AGE OF MENARCHE
Mean (SD) age of menarche was 12.2 (1.8) years (n = 12). There was, however, a wide range (8.9–15.4 years) with the median age being 12 years.
Discussion
The mean birth length of our cohort was increased. Growth remained excessive leading to tall stature (height well above the 97th centile) in the 2nd and 6th years of life. The excessive early growth of our cohort is in agreement with that reported previously.9 ,10Karlberg et al, using the “infancy–childhood–puberty model”, showed that the growth rate in infancy in children with Sotos syndrome was significantly increased.5 This was also associated with later onset of the childhood component of growth. Mean height velocity during the childhood component was similar to controls. Therefore, this pattern of growth leads to a height consistently above the 97th centile in infancy and childhood.
The women had a mean final height within the normal range for the British population. The mean final height for the men was also usually within the normal range, although exceptions to this were more likely than in women. The final heights achieved by both sexes, although within the normal range, were significantly more than their calculated target heights. The women had a target height above the 50th centile whereas the men had a target height below the 50th centile. Furthermore the mean excess in final height compared with target height was greater in the men (11.3 cm) than the women (6.2 cm). This suggests that the final height is more likely to exceed the 97th centile in men with Sotos syndrome than women, although familial growth patterns need to be considered in these estimations.
The age of onset of menarche in most of our postpubertal girls appeared to be early compared with the average age of onset in British girls, which is 13 years,11 although the difference did not reach significance, probably because of the small numbers. The combination of advanced bone age and a tendency to early onset of menarche probably led to a final height in the women, which was on or below the 97th centile. It is important to point out that even the two girls who had a later onset of menarche (at 14 and 15.4 years) did not end up excessively tall.
The excess of span for age and the reduced upper to lower segment body ratio showed that much of the influence on height is a result of limb length.
Endocrinological investigations have not provided an explanation for this growth pattern. There have been individual reports of patients with either hyperthyroidism12 or hypothyroidism,13 but these have been infrequent. Hooket al showed that growth hormone concentrations were adequately suppressed in five of six patients after an oral glucose tolerance test.14 These patients also had a normal increase in growth hormone in response to hypoglycaemia. Reports of insulin-like growth factor I (IGF-I) and IGF-II concentrations have not shown a constant pattern.15-17Amber et al showed that the mean overnight growth hormone concentration of a child with Sotos syndrome aged 1.7 years was high, at 24.6 mU/l. The growth hormone profiles also showed an incomplete return to baseline between pulses. At the age of 3.3 years, the mean serum overnight growth hormone concentrations reduced to 11.5 mU/l, and return to baseline between pulses was more evident. The mean serum overnight hormone concentrations in two other patients with Sotos syndromewho were pubertal were only 4.7 mU/l and 4.2 mU/l, respectively.18 These findings will need to be repeated in a larger number of patients with Sotos syndrome (compared with age and height matched controls) before this can be assumed to be the explanation for the growth pattern in this syndrome.
Other overgrowth syndromes exist and these have occasionally been wrongly diagnosed as Sotos syndrome. In our study, all the patients recruited were examined by the same clinical geneticist with expertise in the syndrome, increasing the likelihood that the data are from a homogenous group.
The fear of gigantic adult height stature is the main reason for offering hormonal treatment (oestrogen/testosterone or somatostatin) to limit final adult height.19 Our study has shown that most patients with Sotos syndrome (especially girls) do not require any intervention to limit adult height.