
Abstract
The great majority of apparently balanced translocations are associated with multiple miscarriages and normal phenotype. Several mechanisms have been proposed to explain how a small percentage of apparently balanced translocations are associated with abnormal phenotypes. One of the proposed mechanisms that have not been well investigated is that apparently balanced translocations may host ‘cryptic’ complex chromosomal rearrangements (CCRs). To test this hypothesis, this study investigated 20 non-preselected cases with apparently balanced translocations in order to determine the presence of cryptic CCRs. Multiprobe subtelomeric and whole chromosome paint FISH analyses revealed and further characterized three cryptic CCRs. Two out of three CCRs showed an unexpected level of complexity. The results of this study provided evidence that the link between an apparently balanced rearrangement and the appearance of abnormal phenotype may be partly explained by the presence of cryptic CCRs. The results also suggested that what is reported as apparently balanced translocation by classical cytogenetics may host cryptic CCRs, which could be more common than initially thought. Furthermore, the use of both of the above-mentioned FISH methodologies was absolutely necessary to detect the CCRs.
Similar content being viewed by others


Introduction
Reciprocal translocations are a mutual exchange between terminal segments from the arm of two chromosomes and are present in 0.1% of the population.1, 2 Although most carriers of balanced translocations are phenotypically normal, an association of cytogenetically balanced translocations with phenotypic abnormalities has been reported.3 The risk of phenotypic abnormality associated with de novo balanced translocations is likely to be due to the chance of chromosome breakage disrupting a gene4 or they may not be truly balanced at the DNA level.5
Families in which a cytogenetically balanced translocation is present in both a normal and a child with a phenotypic anomaly have been a long-standing puzzle for human geneticists. The conventional wisdom has been that if the same balanced karyotype found in the carrier parent and is also detected at prenatal diagnosis, there is no increased risk for phenotypic abnormality in the child. However, Fryns and co-workers claimed an apparent excess of mental and/or physical defects in these translocation children.6 In some of the same rearrangements per se must not be of phenotypical relevance and might just be a coincidental. However, there are reasons to believe that in the majority of the cases there may be an unidentified link between the rearrangement and the abnormal phenotype. Mechanisms proposed to explain this phenomenon include the following: (a) Production of a recessive mutation by the translocation that is expressed when a mutation in the same gene is inherited from the other parent. (b) Far more plausible is the ‘position effects’, with variable expression of a gene or genes near the translocation breakpoint.7 (c) Due to uniparental disomy, an apparently balanced reciprocal translocation transmitted from a carrier parent may be structurally balanced but functionally imbalanced. Due to postconceptional ‘correcting’ loss of the homolog from the normal noncarrier parent, a uniparental disomy will be developed, if the chromosome involved is subject to imprinting.8 (d) If the same rearrangement is found in one parent who is normal, further subtle rearrangements might have occurred during meiosis, for example, through unequal crossing over. (e) The rearrangement is more complex than it seems to be, as the defect is beyond the resolution of routine G-banding techniques. Therefore, cytogenetically apparently balanced translocations may have cryptic complex chromosomal rearrangement that can only be detected by additional methodologies. This hypothesis needs to be further investigated.
We hypothesize that this phenomenon might be more common than was initially thought and requires further investigation. Therefore, in this study we aim to investigate 20 families with cytogenetically apparently balanced translocations in order to determine the presence and frequency of cryptic CCRs.
Materials and methods
Patients and chromosomal analysis
A total of 20 different familial or de novo apparently balanced translocation were included in this study (Table 1). FISH analysis was not carried out previously. The pedigree and the status of familial or de novo for the chromosomal anomaly, as well as the family history and the clinical findings of other members in the family, were determined (Table 1). In Cases No. 1 and 4, all family members with the chromosomal abnormalities are associated with mild mental retardation, while Patient No. 20 is associated with malformations and mental retardation. In Case No. 9 one family member that has the same chromosomal abnormality also has malformations and mental retardation. Case 10 is an unaffected father, who has a son with ‘apparently normal karyotype’, malformations and mental retardation. In all other cases, the abnormalities are associated with multiple miscarriages, including abnormal derivative chromosomal abnormalities in aborted fetuses or children with clinical findings. The chromosomal analysis was carried out or repeated for all or the majority of the other family members using standard methodology for G-banding analysis at the 550–750 band level.
FISH
FISH studies using multiprobe subtelomeric specific probes for all the long and short arm of chromosomes were performed as previously described.9 Whole chromosome paint FISH analysis was performed using the probes and the methodology according to Vysis Co.
Results
Cases 1–6, 13, 14, 17–20 were karyotyped in our lab before 2002 and cases 7 and 15 were initially karyotyped and referred to us from another laboratory. Therefore, chromosomal analysis was repeated in our laboratory for all of these cases, so all-20 cases were recently re-analyzed with G-banding at the 550–750 band level (Table 1). Pedigree and family history were collected in detail and chromosomal analysis was carried out in all family members. This analysis revealed several other members in the families with the same apparently balanced chromosomal abnormality or a related unbalanced translocation.
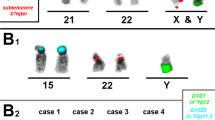
Multisubtelomeric and whole chromosome paint FISH analyses determined additional abnormalities, not previously seen with G-banding analysis, in the cases 10, 15 and 20 (Table 1). Case 10 was reported from different cytogenetic laboratories as an apparently balanced two-way translocation between chromosomes 6 and 7. Multiprobe subtelomeric FISH analysis determined a cryptic three-way translocation with the involvement of the telomeric region of the long arm of chromosome 10 (Figure 1a and b). This abnormality was also detected and confirmed by whole chromosome paint FISH (Figure 1a and b). A small segment of chromosome 10 from 10q26.1–qter was translocated onto chromosome 6q16.2. Chromosome 6 from 6q16.2–qter was translocated onto chromosome 7q34 and the chromosomal region from 7q34–qter was translocated onto chromosome 10q26.1. Case No 15 was originally found by G-banding analysis as an apparently balanced two-way translocation between chromosomes 2 and 3. FISH analyses revealed the involvement of chromosome 15. A very small segment of chromosome 15 from 15q15.1 to 15q15.3 was inserted into the chromosomal region 2q31 and the chromosomal region from 15q15.3 to the telomere was translocated onto chromosome 3q22 (Figure 1c and d). Chromosome 3 from 3q22–qter was translocated onto 2q31 and the chromosomal region from 2q32–qter was translocated onto 15q15.1. The revised karyotype of case 15 includes a CCR with a three-way translocation and an additional small size insertion (Table 1, Figure 1c and d). Case No 20 was originally described by G-banding analysis as a de novo three-way translocation between chromosomes 6, 8 and 12. FISH analyses were performed and identified not only that the above aberration was a four-way translocation, involving chromosome 7 as well, but also revealed additional insertions of very small chromosomal segments. A very small segment of chromosome 7 from 7q32.3–q33 was inserted into chromosome 6p22 and the adjacent larger segment of chromosome 7q33–qter was translocated onto 8q24.21. Another very small segment of chromosome 8 from 8q24.21–q24.22 was also inserted into chromosome 6, proximal to the previously described inserted 7q32.3–q33 segment. The remaining chromosome 8 from 8q24.23–qter was translocated onto chromosome 12q13. Furthermore, chromosome 12 was broken at two sites, at 12p11.2 as well as 12q13. The first segment of chromosome 12 from 12p11.2-pter was translocated onto chromosome 7q32.3 and the second segment from 12q13–qter was translocated onto the abnormal chromosome 6 proximal to the 8q24.22 segment. This very complex karyotype is concluded with the translocation of segment 6p22–pter onto 12p11.2 (Figure 1 e and f). FISH analyses were carried not only in all 20 individuals listed in Table 1 but also in at least one phenotypically normal family member who was a carriers of the same apparently balanced translocation. No CCRs were found in these individuals.

FISH analyses, partial karyotypes and ideograms describing the identified CCRs. (a) Partial karyotypes from multisubtelomeric and whole chromosome paint FISH analyses showing the translocated segments between the chromosomes 6, 7 and 10. (b) Partial karyotypes of G-banded chromosomes and ideograms showing translocated segments between the chromosomes 6, 7 and 10. (c) Partial karyotypes from multi subtelomeric and whole chromosome paint FISH analyses showing the translocated segments between the chromosomes 2, 3 and 15. (d) Partial karyotypes of G-banded chromosomes and ideograms showing translocated segments between the chromosomes 2, 3 and 15. (e) Partial karyotypes from multisubtelomeric and whole chromosome paint FISH analyses showing the translocated segments between the chromosomes 6, 7, 8 and 12. (f) Partial karyotypes of G-banded chromosomes and ideograms showing translocated segments between the chromosomes 6, 7, 8 and 12.

FISH analyses, partial karyotypes and ideograms describing the identified CCRs. (a) Partial karyotypes from multisubtelomeric and whole chromosome paint FISH analyses showing the translocated segments between the chromosomes 6, 7 and 10. (b) Partial karyotypes of G-banded chromosomes and ideograms showing translocated segments between the chromosomes 6, 7 and 10. (c) Partial karyotypes from multi subtelomeric and whole chromosome paint FISH analyses showing the translocated segments between the chromosomes 2, 3 and 15. (d) Partial karyotypes of G-banded chromosomes and ideograms showing translocated segments between the chromosomes 2, 3 and 15. (e) Partial karyotypes from multisubtelomeric and whole chromosome paint FISH analyses showing the translocated segments between the chromosomes 6, 7, 8 and 12. (f) Partial karyotypes of G-banded chromosomes and ideograms showing translocated segments between the chromosomes 6, 7, 8 and 12.
Discussion
In the cytogenetic literature, a number of rearrangements were classified as apparently balanced translocations, however, after further investigation they were determined as CCRs. 10, 11, 12 Investigation with FISH methodologies in the above reports as well as in other studies have been shown to be helpful in resolving these cases, and allowed the identification of cryptic translocated segments.13, 14 This study investigated 20 families with cytogenetically apparently balanced translocation, in order to determine the presence of cryptic CCRs and showed that three of them involved additional rearranged chromosome regions, which finally revised the karyotype as CCR. The results raised the important possibility that apparently balanced translocations may often host cryptic CCRs.
The results of this study suggest that it is highly possible that CCRs might be more common than initially thought. Previous large-scale surveys in newborns,3 as well as in spontaneous abortions,15 suggested that CCRs must be extremely rare. However, with the progress of FISH and other methodologies several families with previously unidentified CCRs have been revealed and reported. In fact, the incidence of subtle rearrangements or CCRs is probably much higher than previously thought,16 as shown by the increasing number of cases that are re-evaluated using FISH techniques.10, 11, 12, 13 On the other hand, it is important to discuss the ‘mode of ascertainment’, as the impact of CCRS and other chromosomal abnormalities is largely underestimated in the literature. Deletions and other chromosomal abnormalities have been reported not to have any association with any phenotypic effect.17 To date, asymptomatic transmitted deletions of at least nine distinct regions of the human genome have been reported.17
This study also emphasizes the need to combine high resolution G-banding with different FISH methodologies. The identification and the precise characterization of CCRs may be difficult or even impossible using only conventional cytogenetic techniques. The first cryptic CCR in case 10 is an unaffected father, who was reported to have an apparently balanced two-way translocation from three different cytogenetic laboratories in different countries. He was referred for chromosomal examination, as he has in his family, one miscarriage and two still births with malformations (all three were not karyotyped), a phenotypically normal daughter with the same apparently balanced two-way translocation as the father, and a severely mentally retarded son with an apparently normal karyotype (karyotyped twice). Before FISH analysis, G-banding analysis of the unaffected father, the unaffected daughter and the mentally retarded son from our laboratory reported again the same findings as previously determined by other cytogenetic laboratories. However, both multiprobe subtelomeric FISH and whole chromosome paint FISH analyses determined a balanced three-way translocation in the unaffected father and daughter and unbalanced cryptic subtelomeric rearrangement in the mentally retarded son. This study is probably the first that demonstrates the presence of a cryptic subtelomeric rearrangement in a three-way translocation that was initially reported as an apparently two-way balanced translocation (Figure 1 a and b). The second family with No 15 was reported by G-banding analysis as two-way reciprocal translocation and not three-way CCR. The missed CCR in this case was probably due to the emphasis given on the anomaly found on the two abnormal chromosomes 2 and 3, and the similarity of bands involved in the later found abnormal segment of chromosome 15. Following identification and characterization of these ‘missed’ anomalies using multiprobe subtelomeric FISH analysis; such abnormalities in many occasions could be identified with high-resolution chromosomal analysis9, 18 (Figure 1 c and d). The third case No 20 was initially reported as apparently three-way translocation by G-banding analysis and it is the only case out of the 20 that is not an apparently balanced two-way translocation. Multisubtelomeric FISH again identified another unknown subtle chromosome abnormality, revealing a four-way chromosomal rearrangement (Figure 1 e and f). It is important to discuss that all three CCRs found were associated with malformations and mental retardation (cases 10, 15, 20) (Table 1). However, three other cases, who were associated with mental retardation (cases 1, 4) or including a family member with malformations and mental retardation (case 9), were found to have no CCRs. It appears that cases with apparently balanced translocation and associated with mental retardation or malformations have higher frequency for cryptic chromosomal abnormalities, but this is not always the associated mechanism. It is also very important to point out that for the last two families (cases 15 and 20), the analysis with whole chromosome paint FISH unexpectedly revealed additional new very small-translocated chromosome segments (Figure 1c,d and 1e,f). These additional subtle rearrangements were not possible to be identified neither by high-resolution G-banding (750 band level) nor multiprobe subtelomeric FISH analysis. The results of this study show that CCRs may often involve additional cryptic chromosomal segments, showing a high degree of complexity. Some translocated chromosomal segments can only be identified by multicolor whole chromosome FISH analysis. Our investigation strongly recommends both FISH analyses in all cases found to have balanced reciprocal translocations or other chromosomal anomalies simple or complex, or unexplained family history and particularly prenatal de novo or familial abnormal karyotypes.
This study provides evidence that apparently balanced translocations classified by G-banding may host additional chromosomal abnormalities and finally defined as CCRs. Such CCRs may have an unexpected level of complexity and may be more common that initially thought. We suggest further investigation and re-evaluation of all cases classified as apparently balanced translocation using at least a combination of multiprobe subtelomeric and whole chromosome paint FISH analyses. The clinical significance of prenatal and postnatal identification of cryptic CCRs is extremely important, as CCRs are associated with reproductive problems, multiple miscarriages, stillbirths or in patients with malformations, mental retardation, dysmorphic features or congenital anomalies. Finally, the findings of this study provide evidence that the unknown link between an apparently balanced rearrangement and the appearance of abnormal phenotype in the family may often explained due to the presence of cryptic CCRs.
References
Jacobs PA, Melville M, Ratcliffe S, Keay AJ, Syme J : A cytogenetic survey of 11,680 newborn infants. Ann Hum Genet 1974; 37: 359–376.
Evans JA, Canning N, Hunter AG et al: A cytogenetic survey of 14,069 newborn infants. III. an analysis of the significance and cytologic behavior of the Robertsonian and reciprocal translocations. Cytogenet Cell Genet 1978; 20: 96–123.
Jacobs PA : Correlation between euploid structural chromosome rearrangements and mental subnormality in humans. Nature 1974; 249: 164–165.
Bonaglia MC, Giorda R, Borgatti R et al: Disruption of the ProSAP2 gene in a t(12;22)(q24.1;q13.3) is associated with the 22q13.3 deletion syndrome. Am J Hum Genet 2001; 69: 261.
Puissant H, Azoulat M, Serre J-L, Piet LL, Junien C : Molecular analysis of a reciprocal translocation t(5;11) (q11;p13) in a WAGR patient. Hum Genet 1988; 79: 280–282.
Fryns JP, Kleczkowska A, Kubien E, Van Den Berghe H : On the excess of mental retardation and/or congenital malformations in apparently balanced reciprocal translocations. A critical review of the Leuven data 1966–1991. Genet Couns 1991; 2: 185–194.
Therman E, Susman M : Human chromosomes: structure, behaviour, and defects. New York: Springer; 1993, 3rd edn, pp 275–276.
Nicholls RD, Knoll JHM, Butler MG, Karam S, Lalande M : Genomic imprinting suggested by maternal heterodisomy in non-deletion Prader–Willi syndrome, 1989. Nature 342: 281–285.
Sismani C, Armour JAL, Flint J, Girgalli C, Regan R, Patsalis PC : Screening for subtelomeric chromosome abnormalities in children with idiopathic mental retardation using multiprobe telomeric FISH and the new MAPH telomeric assay. Eur J Hum Genet 2001; 9: 527–532.
Delaroche I, Sabani M, Calabrese G, Mingarelli R, Palka G, Dallapiccola B : Fetal translocation between chromosomes 2, 18 and 21 resolved by FISH. Prenat Diagn 1995; 15: 278–281.
Fuster C, Miguez L, Miro R, Rigola MA, Perez A, Egozcue J : Familial complex chromosome rearrangement ascertained by in situ hybridization. J Med Genet 1997; 34: 164–166.
Petit P, Devriendt K, Vermeesch JR, De Cock P, Fryns JP : Unusual de novo t(13;15)(q12.1;p13) translocation leading to complex mosaicism including jumping translocation. Ann Genet 1998; 41: 22.
Batista DA, Tuck-Muller CM, Martinez JE, Kearns WG, Pearson PL, Stetten G : A complex chromosomal rearrangement detected prenatally and studied by fluorescence in situ hybridization. Hum Genet 1993; 92: 117–121.
Wieczorek D, Engels H, Viersbach R, Henke B, Schwanitz G, Passarge E : Analysis of a familial three-way translocation involving chromosomes 3q, 6q, and 15q by high resolution banding and fluorescent in situ hybridisation (FISH) shows two different unbalanced karyotypes in sibs. J Med Genet 1998; 35: 545–553.
Braekeleer MD, Dao TN : Cytogenetic studies in couples experiencing repeated pregnancy losses. Hum Reprod 1990; 5: 519–528.
Wakita Y, Narahara K, Tsuji K et al: De novo complex chromosome rearrangement in identical twins with multiple congenital anomalies. Hum Genet 1992; 88: 596–598.
Sumption N, Barber JCK : A transmitted deletion of 2q13 to 2q14.1 causes no phenotypic abnormalities. J Med Genet 2001; 38: 125–126.
Giardino D, Finelli P, Gottardi G et al: Cryptic subtoleric translocation t(2;16) (q37;q24) segregating in a family with unexplained stillbirths and a dysmorphic, slightly retarded child. Eur J Hum Genet 2001; 9: 881–886.
Acknowledgements
The study was funded by the Fifth European Union ‘EURO-MRX’ program QLG3-CT-2002-01810.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Patsalis, P., Evangelidou, P., Charalambous, S. et al. Fluorescence in situ hybridization characterization of apparently balanced translocation reveals cryptic complex chromosomal rearrangements with unexpected level of complexity. Eur J Hum Genet 12, 647–653 (2004). https://doi.org/10.1038/sj.ejhg.5201211
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.ejhg.5201211
Keywords
This article is cited by
-
Cryptic breakpoint identified by whole-genome mate-pair sequencing in a rare paternally inherited complex chromosomal rearrangement
Molecular Cytogenetics (2018)
-
Characterization of a complex rearrangement involving chromosomes 1, 4 and 8 by fish and array-CGH
Journal of Applied Genetics (2012)
-
Clinical application of whole-genome array CGH during prenatal diagnosis: Study of 25 selected pregnancies with abnormal ultrasound findings or apparently balanced structural aberrations
Molecular Cytogenetics (2010)
-
Application of molecular cytogenetic techniques to clarify apparently balanced complex chromosomal rearrangements in two patients with an abnormal phenotype: case report
Molecular Cytogenetics (2009)
-
Cryptic genomic imbalances in patients with de novo or familial apparently balanced translocations and abnormal phenotype
Molecular Cytogenetics (2008)
