Article Text

Abstract
Germline CDH1 mutations confer a high lifetime risk of developing diffuse gastric (DGC) and lobular breast cancer (LBC). A multidisciplinary workshop was organised to discuss genetic testing, surgery, surveillance strategies, pathology reporting and the patient's perspective on multiple aspects, including diet post gastrectomy. The updated guidelines include revised CDH1 testing criteria (taking into account first-degree and second-degree relatives): (1) families with two or more patients with gastric cancer at any age, one confirmed DGC; (2) individuals with DGC before the age of 40 and (3) families with diagnoses of both DGC and LBC (one diagnosis before the age of 50). Additionally, CDH1 testing could be considered in patients with bilateral or familial LBC before the age of 50, patients with DGC and cleft lip/palate, and those with precursor lesions for signet ring cell carcinoma. Given the high mortality associated with invasive disease, prophylactic total gastrectomy at a centre of expertise is advised for individuals with pathogenic CDH1 mutations. Breast cancer surveillance with annual breast MRI starting at age 30 for women with a CDH1 mutation is recommended. Standardised endoscopic surveillance in experienced centres is recommended for those opting not to have gastrectomy at the current time, those with CDH1 variants of uncertain significance and those that fulfil hereditary DGC criteria without germline CDH1 mutations. Expert histopathological confirmation of (early) signet ring cell carcinoma is recommended. The impact of gastrectomy and mastectomy should not be underestimated; these can have severe consequences on a psychological, physiological and metabolic level. Nutritional problems should be carefully monitored.
- Cancer: gastric
- Clinical genetics
- Diagnostics
- Cancer: breast
- Stomach and duodenum
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Introduction
Worldwide, gastric cancer (GC) is the fifth leading cause of cancer and the third most common cause of death from cancer, with an estimated number of 723 000 deaths annually.1 The vast majority of GCs are sporadic, but it has now been established that 1–3% of GCs arise as a result of inherited cancer predisposition syndromes. These syndromes include Li-Fraumeni syndrome,2–4 Lynch syndrome,5–7 Peutz-Jeghers syndrome,8–10 hereditary breast and ovarian cancer,11 ,12 MUTYH-associated adenomatous polyposis (MAP),13 familial adenomatous polyposis,14–16 juvenile polyposis syndrome17 ,18 and PTEN hamartoma tumour syndrome (Cowden syndrome).19 The lifetime risk of GC in these syndromes varies substantially between populations studied, but is generally low.
Over 15 years ago, linkage analysis implicated germline mutations in the CDH1 gene, encoding the tumour-suppressor protein E-cadherin, as the genetic cause of hereditary diffuse GC (HDGC).20 Heterozygous germline CDH1 mutations increase lifetime risk of developing diffuse GC (DGC) and lobular breast cancer (LBC). Criteria have been set to select families eligible for screening of germline CDH1 mutations, and they were updated in 2010.21 ,22 Not all families fulfilling these criteria have mutations in CDH1, indicating that other genes may also be involved in DGC predisposition. Germline mutations in CTNNA1 were described in three families that presented with DGC, one of them fulfilled the 2010 HDGC criteria.23 ,24
Increasing awareness of HDGC and the rapid advances in genetic diagnostic tools, endoscopic modalities and the increasing use of laparoscopic surgery led a group of clinical geneticists, gastroenterologists, surgeons, oncologists, pathologists, molecular biologists, dieticians and patients' representatives from nine different countries to convene a workshop in order to update the management guidelines for this condition set in 2010 and to propose directions for future research. The workshop discussions were focused on five major topics: (1) genetic counselling and mutation analysis; (2) endoscopic surveillance and screening of cancer; (3) risk-reduction surgery of the stomach and breasts; (4) pathological specimen processing and diagnosis; and (5) patients' and dieticians' perspective.
Genetic counselling and mutation analysis
Genetic evaluation of patients with HDGC
Genetic counselling is an essential component of the evaluation and management of HDGC. The counselling process should include a formal genetics evaluation by a cancer genetics professional with expertise in the field. The evaluation should include a detailed three-generation family pedigree, histopathological confirmation of DGC diagnoses and/or precursor lesions (in situ or pagetoid spreading of signet ring cells) and a discussion on lifetime risks of developing DGC and LBC. Informed consent for genetic testing is required. In the management of individuals with a CDH1 mutation, a full multidisciplinary team (MDT) should be involved comprising those with relevant expertise in gastric surgery, gastroenterology, breast oncology, pathology, psychosocial support and nutrition. Genetic testing can be offered from the age of consent (and therefore will vary between countries, but will generally be around 16–18 years). Testing of younger unaffected family members can be considered on a case-by-case basis. Rare cases of clinically significant DGC have been reported in affected families before the age of 18,25 but the overall risk of this disease before the age of 20 is low.26 ,27
Cancer risks in CDH1 mutation carriers
In a recent study, penetrance data for CDH1 mutation carriers has been updated based on affected individuals, who presented clinically with DGC or LBC, from 75 families with pathogenic CDH1 mutations. Families with CDH1 missense mutations and families for which no carrier test information was available were excluded from this analysis. The cumulative risk of DGC for CDH1 mutation carriers by age 80 years is reported to be 70% for men (95% CI 59% to 80%) and 56% for women (95% CI 44% to 69%). Furthermore, the cumulative risk of LBC for women with a CDH1 mutation is estimated to be 42% (95% CI 23% to 68%) by 80 years. There is currently no evidence that the risk of other cancer types in individuals with a CDH1 mutation is significantly increased.24
Implications of counselling
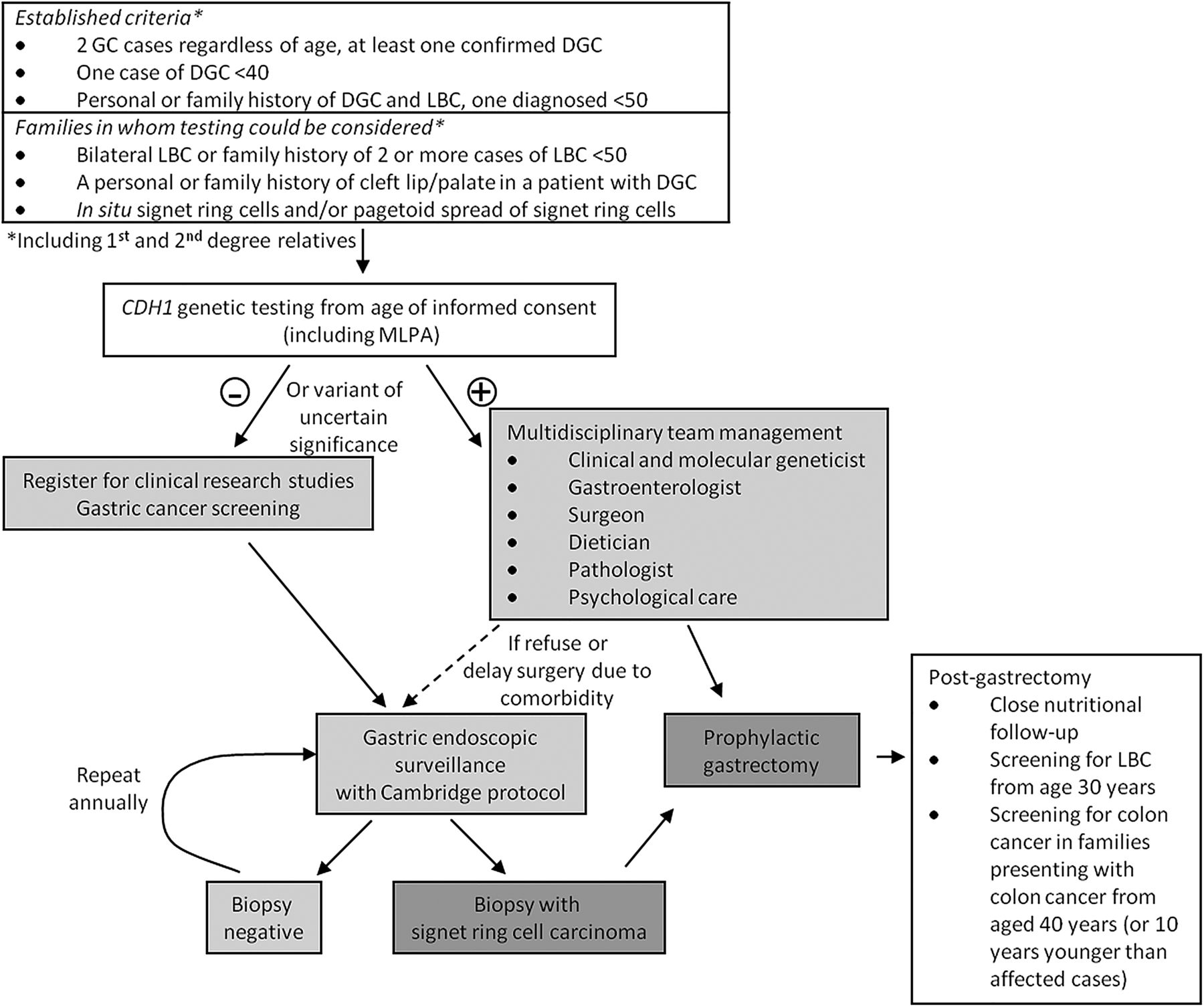
Clinical geneticists (or other members of the MDT) should inform the counselee about gastric surgery and options of surveillance. Proven pathogenic CDH1 germline mutation carriers should be advised to undergo prophylactic gastrectomy (for more details, see the ‘Surgery’ section). Some patients may want to delay prophylactic gastrectomy for personal and/or work-related reasons. In these individuals, endoscopic surveillance, described in detail under the ‘Endoscopic surveillance’ section, should be considered in the interim. The management of patients and families with clinical features suggestive of HDGC, but without a germline CDH1 mutation, is not straightforward. We advise intensive endoscopic surveillance in an expert centre for first-degree relatives of patients meeting criteria mentioned in figure 1. This is also the case for patients and families who carry a CDH1 variant with unproven deleterious effect. Recommendations on breast cancer surveillance and therapy in CDH1 mutation carriers can be found below.

Algorithm for management starting from clinical hereditary diffuse gastric cancer (HDGC) testing criteria, genetic testing, role of endoscopy and gastrectomy. GC, gastric cancer; DGC, diffuse gastric cancer; LBC, lobular breast cancer; MLPA, multiplex-ligation probe amplification.
Criteria for germline CDH1 mutation testing
The last guideline in 2010 broadened the clinical criteria to select patients eligible for CDH1 mutation analysis. The detection rate of CDH1 mutations before 2010, using the guidelines established in 1999,21 was reported to be 25–50%.27 ,28 Using the new criteria, the CDH1 detection rate in countries with a low incidence of GC has decreased to 10–18% (RS van der Post et al, under revision, 2015).24 ,29 This decrease may also be explained partly by the enrichment of large and highly suspected families in studies published before 2010 (ie, ascertainment bias). The detection rate is considerably higher in the New Zealand Maori population and is likely higher in the Newfoundland population, where a founder mutation has been described.27 It should be noted that these criteria are designed for countries with a low incidence of sporadic GC. Few small series and case reports of individuals with CDH1 mutations have been described in countries with a high incidence of sporadic GC; no large cohorts were examined systematically. In small series of South Korea, Japan and Portugal, mutation detection rates of pathogenic germline CDH1 mutations in HDGC and early-onset GC range between 8% and 15%.2 ,30–33
During the workshop, it was decided to merge the first (‘Two or more GC cases in a family, one DGC <50’) and second (‘Three or more DGC cases regardless of age’) testing criteria from the previous guideline22 into a new criterion: ‘Two or more GC cases regardless of age, at least one confirmed DGC’, in first-degree and second-degree relatives. The two other testing criteria have not been changed. The revised criteria are depicted in the upper panel of the box in figure 1. The revised criterion now covers families for whom detailed pathology is incomplete. However, as in the earlier criteria, confirmed intestinal-type GC cases are not part of HDGC and in these families no CDH1 mutation analysis should be performed. To properly assess whether a family meets the HDGC criteria, pathology reports and preferably review of gastric specimens by a pathologist dedicated to GC are essential.
There are other families in which genetic testing may also be considered (figure 1, lower panel). The presence of bilateral LBC at young age (under the age of 50 years) or the presence of multiple close relatives with LBC (at least two under the age of 50 years) may justify testing for CDH1 mutations.29 ,34 Testing should also be considered in individuals with a personal or family history of cleft lip/cleft palate and DGC.35 ,36 Furthermore, in cases where expert pathologists detect in situ signet ring cells and/or pagetoid spread of signet ring cells in the stomach, genetic testing should be considered since this is rarely (if ever) seen in sporadic cases. Genetic testing should, whenever possible, be initiated in an affected proband. If the affected proband is deceased, frozen-fixed or formalin-fixed, paraffin-embedded tissue (preferably normal, non-malignant tissue) still may be available for CDH1 germline mutation testing. In case tissue of an affected individual is not available or of insufficient quality to perform the test, testing of unaffected relatives is acceptable. This should be performed preferably in at least three first-degree relatives simultaneously, thus increasing the likelihood of detecting a CDH1 mutation. However, it has to be made clear to the counselee that unaffected individuals have only a 50% chance of having inherited a mutated CDH1 allele. The testing criteria still have to be met by the counselee's family. If no mutation is found in these cases, endoscopic screening should be discussed with an expert gastroenterologist on a case-by-case basis. Similarly, in small families with DGC or in families where family history is unavailable, CDH1 mutation screening should also be considered on a case-by-case basis.
Genetic testing: lab perspective
Genetic testing on blood or tissue for germline mutations should be performed in certified molecular diagnostic laboratories, for example, Clinical Laboratory Improvement Amendments approved, ISO 15189 accredited or equivalent. CDH1 analysis should include mutation analysis of the entire open-reading frame, including intron–exon boundaries, as well as copy number analysis of individual exons to detect intragenic exon deletions or duplications. At present, analyses are mostly performed by a combination of Sanger sequencing and Multiplex Ligation-dependent Probe Amplification. These techniques can be replaced by next-generation sequencing if the approach used fulfils the requirement of similar sensitivity.
To date, over 155 different germline CDH1 mutations have been described, the majority pathogenic mutations and a number of variants of uncertain significance (RS van der Post et al, under revision, 2015).24 The majority of the pathogenic mutations are truncating and thus do not lead to a functional protein. Large exonic deletions are relatively rare, with a frequency of about 5%.37 ,38 CDH1 is a tumour suppressor gene and therefore a somatic second hit is required for initiation of tumour formation. The trigger and molecular mechanism by which the second allele of CDH1 is inactivated appears to be diverse and includes methylation, somatic mutation and loss of heterozygosity.39–42
The identification of germline CDH1 missense variants requires additional studies to assess their putative pathogenicity. A multidisciplinary approach combining familial and population data, in silico analysis and in vitro analysis is currently used to classify the variants as neutral or pathogenic.43–47 Genetic parameters such as mutation frequency in healthy control populations, co-segregation of the mutation within the pedigree and recurrence of the mutation in independent families should be considered as a first approach.43 ,45 However, the low number of individuals affected by the disease, the small size of the pedigrees and the absence of mutation hotspots (which prevents the establishment of any correlation between the mutation site and its functional consequence) are limitations of this approach. In silico experiments predict the degree of conservation of a specific nucleotide within species, the effect of missense variants on splicing and also the putative impact of the variants on protein structure.45 ,47 Still, in silico results should be carefully interpreted because the degree of conservation among species of each amino acid position is considered separately and does not take into account possible compensatory effects of neighbouring amino acids.45 ,47 Functional in vitro assays should be performed in order to evaluate the impact of CDH1 missense alterations in protein structure, trafficking, signalling and, consequently, in E-cadherin function.44 ,46 When compared with the cells expressing wild-type E-cadherin, pathogenic missense mutants impair the correct binding of key adhesion-complex regulators and likely compromise normal E-cadherin localisation and stability at the plasma membrane.46 ,48 As a consequence, disruption of cell–cell adhesion and increased invasive behaviour may be observed in the presence of pathogenic variants.44 ,46 To date, 49 germline CDH1 missense variants were reported for functional evaluation to Institute of Molecular Pathology and Immunology of the University of Porto (Portugal, reference laboratory for functional characterisation of CDH1 missense variants for the International Gastric Cancer Linkage Consortium), the majority being classified as deleterious and thus possibly pathogenic (R Seruca, personal communication, 2014).
Panel sequencing
Penetrance estimates for CDH1 mutation carriers have been derived from the study of highly ascertained HDGC families and it is likely that the penetrance for mutations detected in non-HDGC families will be lower. With the introduction of next-generation sequencing-based gene panels, both in research and diagnostic settings, CDH1 alterations may be found in patients without a personal or family history of GC.49 ,50 In our opinion, one should be very cautious in the interpretation of coding variants identified in non-HDGC families, especially if the alterations do not lead to a premature stop codon.
CDH1 mutation database
Currently, there is no international database containing all germline CDH1 mutations and variants identified to date. A database has been designed and is currently under construction with the collaboration of the LOVD team. The variant database is available at http://www.LOVD.nl/CDH1. This database can be consulted to assess whether a given CDH1 mutation has been found by others and whether it has been considered deleterious and likely disease-causative or not based on population data, segregation analysis, in silico analysis and in vitro functional analysis, and/or recurrence in several individuals/families. We advise researchers and clinicians to submit unpublished mutations and variants to the database (contact C Oliveira, carlaol@ipatimup.pt), together with the requested information on families/patients and mutations. The publication/submitter of every mutation will always be referred to in the database.
Psychosocial effects of counselling
Even though it is well recognised that many individuals will benefit from genetic counselling and testing for hereditary cancer in general, there have also been reports that it may induce a number of psychosocial problems. In a review on individuals requesting genetic counselling and testing for hereditary cancer syndromes, six dominant problem areas were identified: (1) coping with cancer risk; (2) practical problems (such as obtaining life insurance/loans and employment when found to be a mutation carrier); (3) family-related problems (eg, communication problems with family members, feeling responsible for family members); (4) children-related problems (eg, concerns for children having increased risk, fear of leaving young children); (5) living with cancer (eg, fear of developing cancer, pain about the loss of family members) and (6) emotions (eg, anxiety, anger, feelings of loss, but also relief and reassurance).51 These topics, when applicable, should be addressed during the counselling sessions.
Pregnancy and assisted reproduction
Although scientific data are lacking concerning timing of prophylactic gastrectomy and family planning, it is entirely possible for women to give birth to a healthy child after gastrectomy.52 Nutritional advice and follow-up with a dietician within this context is essential.
Individuals from hereditary cancer families are frequently concerned about the transmission of their predisposition of cancer to their children.53 ,54 Healthcare professionals, including geneticists and psychosocial workers, will be increasingly involved in discussions and decisional counselling regarding reproductive options in families with a known cancer predisposing mutation such as CDH1. In the past decades, genetic testing for hereditary cancers before birth has become available through prenatal diagnosis (PND) and preimplantation genetic diagnosis (PGD).55 We recommend that carriers of a CDH1 mutation with a desire to have children should be informed about all reproductive options, including PND and PGD.
Future research: other genes involved in HDGC predisposition
Currently, three families that meet the new criteria have been described to carry germline CTNNA1 mutations.23 ,24 Even though these families show a clinical picture similar to that of CDH1 mutation-positive families,23 insufficient data are available to make a statement on disease penetrance. Given the functional connection between the two genes, they may represent a genocopy. Mutation carriers could be given the option of prophylactic total gastrectomy (PTG) and other cancer prevention measures recommended for HDGC families, but with the precaution that such advice is being given based on very limited data.
Other families have recently been described with BRCA2 and PALB2 mutations;24 however, we recommend that these families are managed no differently than other families with such mutations according to national guidelines. It is likely that other HDGC-associated genes will be discovered through whole exome, genome or other unbiased next-generation-sequencing empowered methodologies. Indeed, using a combination of this approach and linkage analysis, mutations in MAP3K6 have recently been described.56 More needs to be understood about families with MAP3K6 mutations before they could be used to stratify risk in families. Until such data are available, a cautious approach in which all first-degree relatives of mutation carriers are followed is recommended. Without multiple mutation-positive families for newly identified genes, it will be extremely difficult to ascribe pathogenicity to such mutations and to develop management guidelines.
Screening and surveillance
Gastric endoscopic screening and surveillance
To clarify the terminology, we consider that individuals having endoscopy who do not know their mutation status or those who do not have a proven pathogenic CDH1 mutation undergo screening whereas mutation-positive individuals undergo surveillance. The consensus reached at the workshop was that individuals who tested positive for a pathogenic germline CDH1 mutation should be advised to consider prophylactic gastrectomy, regardless of endoscopic findings. However, the timing of surgery may vary according to the preferences and age, as well as the physical and psychological fitness of the individual. In patients proceeding for gastrectomy, a baseline endoscopy should be performed prior to surgery to look for macroscopic tumour as this may alter the treatment plan. This endoscopy is also performed to ensure that there is no other coincidental pathology, such as Barrett's oesophagus, which may alter the extent of the resection. When the stomach is macroscopically normal, the information on microscopic disease foci is useful to compare with findings in the surgical resection specimen and hence to increase knowledge on the likelihood of endoscopic detection of microscopic lesions.
For individuals with a CDH1 mutation in whom gastrectomy is not currently being pursued (eg, through patient choice or existence of physical or psychological comorbidity), regular endoscopy should be offered. In patients declining surgery, surveillance can have the advantage of helping individuals to come to a decision about the need for gastrectomy when microscopic foci of signet ring cells are detected. However, patients should be aware that delaying surgery can be a hazardous decision.57
The management of individuals with a CDH1 variant of uncertain significance and those in whom no mutation can be identified in the family is not straightforward. We would recommend that intensive endoscopic surveillance in an expert centre should be offered to these families who fulfil the HDGC criteria. Endoscopic screening has a valuable role in guiding clinical decision making and in one case series lesions were detected in 2/7 CDH1 mutation-negative individuals (1/5 families).57 Specifically, any malignant lesions detected endoscopically would prompt a referral for gastrectomy. However, all patients undergoing endoscopy for HDGC should be informed that, given the very focal and often endoscopically invisible nature of these lesions, it is quite possible that lesions will not be detected by random biopsies.
HDGC endoscopy protocol
Endoscopy should be performed in centres with an experienced MDT. However, it is appreciated that sometimes this is not practical for individuals who have to travel long distances. In this case, a local endoscopist in consultation with an expert centre on the endoscopy protocol and review of histology may be a helpful alternative.
As noted above, the optimal frequency of endoscopy is not known. Based on current experience, it is recommended that individuals should be offered annual endoscopy. The bleeding risk may be slightly higher than for other indications since more biopsies are taken. Therefore, it is recommended that the local high-risk endoscopy protocol is followed such that, if possible, anticoagulants (eg, warfarin and clopidogrel) are stopped prior to the procedure. The endoscopy should be performed using a white light high definition endoscope in a dedicated session of at least 30 min to allow for careful inspection of the mucosa on repeated inflation and deflation and for collection of biopsies. The mucosa should be thoroughly washed before examination with a combination of mucolytics (N-acetylcysteine) and antifoaming agent (such as simethicone) mixed with sterile water. This washing is ideally done via a pump operated by a foot pedal. The macroscopic appearances of the gastric mucosa and any focal visible lesions should be recorded using still images or video for future reference and specifically sampled for histology prior to the collection of random biopsies.
Prior to examination for small foci, the stomach should be adequately inflated and deflated to check distensibility. Poor distensibility should raise alarm for a submucosal infiltrative process like linitis plastica. When this is the case, biopsies should be taken and further imaging such as a high-resolution multidetector CT scan combined with endoscopic ultrasonography is suggested to visualise the gastric wall layers. No objective measures of distensibility are currently available, and this is an area that may warrant future research.
Although an association between Helicobacter pylori infection and HDGC has not been proven, it is important to test for H. pylori to document the prevalence of infection. Since H. pylori is a WHO class 1 carcinogen, it is agreed that when individuals are infected it should be eradicated, especially in those opting for surveillance. A rapid urease test is the preferred test at baseline, and additionally, it is recommended to take random biopsies from the antrum and the corpus due to patchy colonisation, especially in the presence of acid suppression.
Due to the tiny foci of signet ring cells, which can only be recognised by microscopy, multiple biopsies are required to maximise the likelihood of diagnosing them.39 The anatomical gastric localisation in which foci are identified varies between studies; reasons for this remain to be clarified but may include environmental factors or differences in the molecular pathogenesis.39 ,57–65 Therefore, it is recommended that any endoscopically visible lesions are biopsied including pale areas. Additionally, random sampling should be performed comprising five biopsies taken from each of the following anatomical zones: pre-pyloric area, antrum, transitional zone, body, fundus and cardia. A minimum of 30 biopsies is recommended as described in the Cambridge protocol (see online supplementary protocol 1).22 Even though this will still lead to sampling bias due to the large gastric surface area, taking more biopsies is not feasible in practice.65 The biopsies may be taken using a standard forceps, ideally with a spike as this will seize the lamina propria in which signet ring cell foci are present. In the case of a well-defined visible lesion, an endoscopic mucosal resection can be helpful to achieve a more reliable histopathological specimen to document the degree of invasion. However, this should be done for diagnostic rather than therapeutic purposes in view of the multifocal nature of the lesions.
Special mention should be given to pale areas since these are more likely to harbour microscopic foci of abnormal cells, although they lack specificity leading to false positives (figure 2).66 Recent data also suggest that these areas are visible on careful examination by white light, but narrow band imaging may make them easier to visualise (A Cats, personal communication, 2014). As noted in the previous guidelines, chromoendoscopy with Congo-red and methylene blue is no longer recommended due to concerns over toxicity.66 Virtual chromoendoscopy using autofluorescence and trimodal imaging does not seem to confer much additional benefit over white light.57 In order to maximise the yield from endoscopy, specialist histopathology reporting is essential and the guidelines outlined in the pathology section below should be followed.

Pale areas in gastric mucosa of a patient with a germline CDH1 mutation harbouring signet ring cell focus during white light endoscopy (A) and narrow band imaging (B). H&E stain of biopsy specimen with signet ring cells (C). Scar area after biopsy during previous endoscopy (D).
Endoscopic surveillance of colorectal cancer
Although there are case reports of colorectal and appendiceal signet ring cell carcinomas (SRCCs) in CDH1 mutation carriers,26 ,67–70 there is currently no evidence to suggest that the risk of colorectal cancer in CDH1 mutation carriers is significantly elevated and there are insufficient data to give recommendations on colorectal cancer screening. In CDH1 mutation families in which colon cancer is reported in mutation carriers, information should be collected concerning the age at diagnosis, whether the affected member(s) and first-degree or second-degree relatives are mutation carriers and whether the histopathology showed a mucinous component and/or signet ring cells. For such families, enhanced colonoscopy screening should be considered at age 40 or 10 years younger than the youngest diagnosis of colon cancer, whichever is younger, and repeated at intervals of 3–5 years. In the absence of a family history, the national guidelines for colon cancer screening should be followed. It is imperative that data on colonoscopic screening in these individuals are collected so that these guidelines can be based more on evidence than on specialist opinion in the future.
Breast cancer surveillance
Knowledge about breast cancer risk in HDGC has slowly advanced since first reported in 2000,26 yet evidence is not sufficient such that recommendations can be made of comparable strength as in BRCA1/2. Genotype–phenotype correlations may eventually show some HDGC families do not have an increased LBC risk, but at present it should be assumed all women with a CDH1 mutation are at risk. When informing women with CDH1 mutation about the role of breast surveillance versus prophylactic mastectomy to manage their risk, the consultation covers similar territory as in BRCA1/2. There are, however, some important differences that must be carefully explained.
Invasive LBC, the type that typically occurs in HDGC, makes up 5–15% of sporadic breast cancer. Invasive ductal cancer occurs in 85–95% of sporadic breast cancer and in BRCA1/2 cases.71 In contrast to ductal breast cancer, E-cadherin-deficient LBC invades in sheets or cords of cells, typically in single file, and does not form a well-defined mass. Studies comparing different radiological modalities in sporadic LBC show sensitivity on mammography ranges from 34% to 92%.71 Bilateral breast MRI needs to be part of the protocol in CDH1 mutation carriers. Given the fact that mammography has a low sensitivity for LBC, synchronous mammography at the time of MRI may add little. We therefore recommend annual breast MRI (which can be combined with mammography) starting at age 30 in women with a CDH1 mutation. An oncologist or breast surgeon should guide breast surveillance. Annual clinical breast examination and breast cancer awareness from the patient and her physicians are essential.
Future research on gastric and breast surveillance
In light of emerging endoscopic technologies, such as narrow band imaging, blue laser imaging, I scan, autofluorescence imaging, IHb-enhancement and confocal endomicroscopy,72 research is required to further study the optimal methods for endoscopic monitoring of individuals at risk for DGC. Given the rarity of this condition, these need to be multicentre studies with strictly defined protocols. In addition, it is likely that the multiple biopsy protocol leads to scarring that can masquerade as pale areas (figure 2D). It would therefore be very valuable to compare the yield of a targeted biopsy approach only with the current Cambridge protocol, which also includes multiple random biopsies. Such studies could also inform on the interobserver variation in the identification of pale areas and help define features indicative of a signet ring cell focus. An endoscopic atlas created by endoscopists performing regular endoscopies on CDH1 mutation carriers would be very useful to help standardise protocols and improve lesion recognition.
There are no studies specifically addressing screening for LBC. Trials on breast screening in the general population and MRI screening in high-risk groups or BRCA1/2 are informative but do not directly extrapolate to the screening scenario in HDGC. The outcomes of the above-stated recommendations of breast surveillance in HDGC women should be further prospectively investigated.
Gastrectomy and mastectomy
Prophylactic gastrectomy: indications for and timing of surgery
Prophylactic gastrectomy should be strongly advised in carriers of a proven pathogenic germline CDH1 mutation. Some argue that the term ‘prophylactic gastrectomy’ is inaccurate and favour the term ‘risk reduction gastrectomy’ because most mutation carriers already have microscopic SRCCs at the time of their surgery. Total gastrectomy for these patients, however, completely eliminates their risk of GC and is truly prophylactic in terms of preventing their death from invasive GC.
The optimal timing of prophylactic gastrectomy is unknown and is usually highly individualised. Since this surgery has major impact on the quality of life, the decision to undergo prophylactic gastrectomy should be well informed, balanced, prepared and timed. Decisional counselling, outweighing the pros and the cons of the intervention is essential. The current consensus is that the procedure should be discussed and offered to pathogenic germline CDH1 mutation carriers in early adulthood, generally between ages 20 and 30.58 Based upon the physical fitness of the mutation carrier and of surgery-related complications, prophylactic gastrectomy at an age >75 should be carefully considered. Family phenotype, especially age of onset of clinical cancer in probands, should be taken into account. There is likely to be a dormant period in which the signet ring cell adenocarcinoma does not spread or progress since they have a low proliferative index and the age of prophylactic gastrectomy is generally lower than that of overt cancer.39 This may explain why so many individuals are found to have T-1 N-0 stage tumours after prophylactic gastrectomy.73 Patients who develop symptomatic, widely invasive DGC have a poor prognosis with as few as 10% having potentially curable disease.74 Even if potentially curable, 5-year survival rate still does not exceed 30%.75 As our understanding of the natural history of mucosal SRCC improves, it may be possible to safely postpone prophylactic gastrectomy in some patients, but until such time it is safer to recommend surgery early in adult life. This has implications for the long-term follow-up of patients with prophylactic gastrectomy and reinforces the need for MDTs to care for these patients for the rest of their lives, similar to patients who have undergone bariatric malabsorptive surgery for obesity.76
Operation details
The requisite operation is a total gastrectomy with Roux-en-Y reconstruction, ensuring that the jejunojejunal anastomosis is at least 50 cm distal to the oesophagogastric anastomosis, to reduce the risk of biliary reflux. The proximal resection line must be across the distal oesophagus containing squamous epithelium to ensure that no gastric cardiac mucosa is left behind. This can be confirmed by frozen section or examination of the opened resection specimen in operating room, and can be guided by the use of on-table endoscopy to mark the squamocolumnar junction during the surgery.
The optimal extent of lymph node dissection (LND) in prophylactic gastrectomy is controversial.77 Lymph node metastases are not reported in asymptomatic CDH1 mutation carriers with negative preoperative surveillance biopsies or small foci of pT1a intramucosal carcinoma. Among patients with early-stage intestinal adenocarcinoma of the stomach, the frequency of lymph node metastasis in patients with early intramucosal (pT1a) tumours is 2–5%,78–81 and up to 6% in the undifferentiated or diffuse types.78 ,80 In pT1b tumours, with invasion of the submucosal layer, lymph node metastases are found in 17–28%, increasing with the depth of submucosal invasion.80 ,81 The majority of patients undergoing prophylactic gastrectomy for HDGC will have at least T1a cancers. Because a preoperative gastroduodenoscopy cannot exclude the presence of T1b lesions with their higher risk of metastases during the operation, a D1 LND (with the inclusion of lymph node stations 1–7) is reasonable.
The formation of a jejunal pouch may improve eating for the first year after surgery, but, as yet, prospective trials comparing pouch to straight Roux-en-Y reconstruction have not convincingly demonstrated significant long-term benefits to justify the routine application of this more complex reconstructive procedure.82 Surgeons should therefore use the reconstruction they are most familiar with. This also applies to whether the preferred surgical approach is open or laparoscopic.77 ,83 There are potential advantages of laparoscopic gastrectomy with reduced wound pain and faster overall return to full activities, but conclusive evidence for the superiority of this approach is still lacking. Any surgeon proposing to do a laparoscopic PTG must be able to reassure the patient that this is without additional risk compared with open surgery.
Prophylactic mastectomy
Prophylactic mastectomy is not routinely recommended but may be a reasonable option for some women. Literature about prophylactic mastectomy in HDGC is scarce, and it is reasonable to consider prophylactic mastectomy on a case-by-case basis taking into account the family pedigree. National guidelines for high-risk women should be followed with respect to chemoprevention using selective oestrogen receptor modulators or aromatase inhibitors.
Histopathology
Histopathology of biopsies from individuals suspected for HDGC
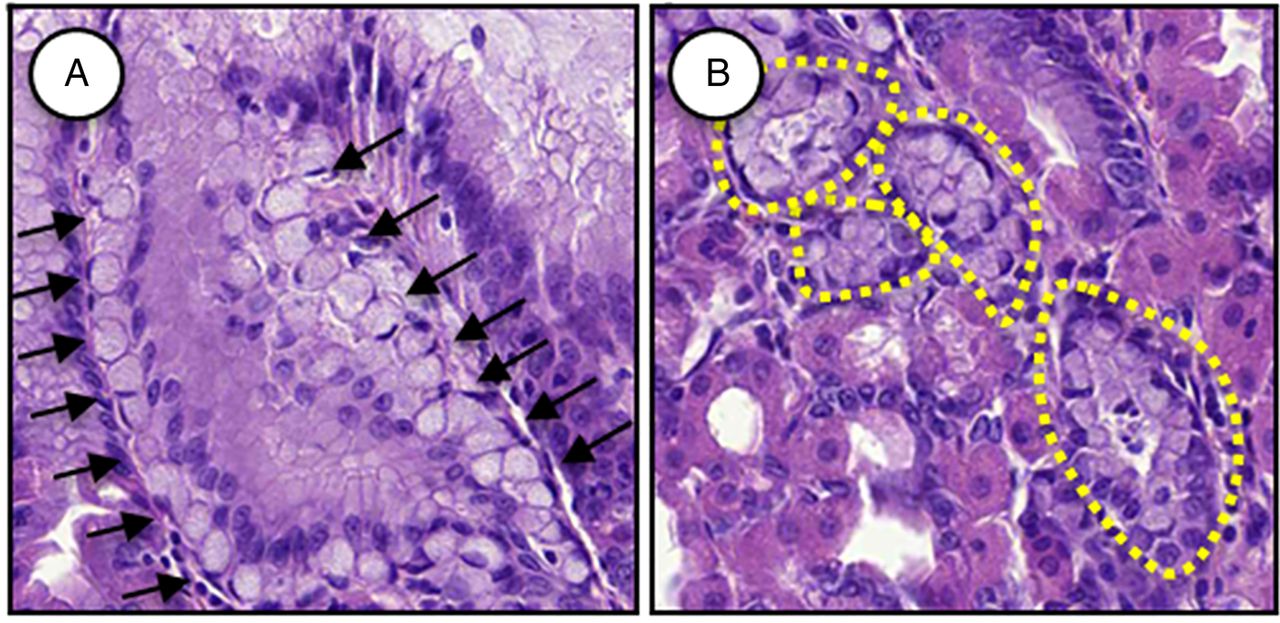
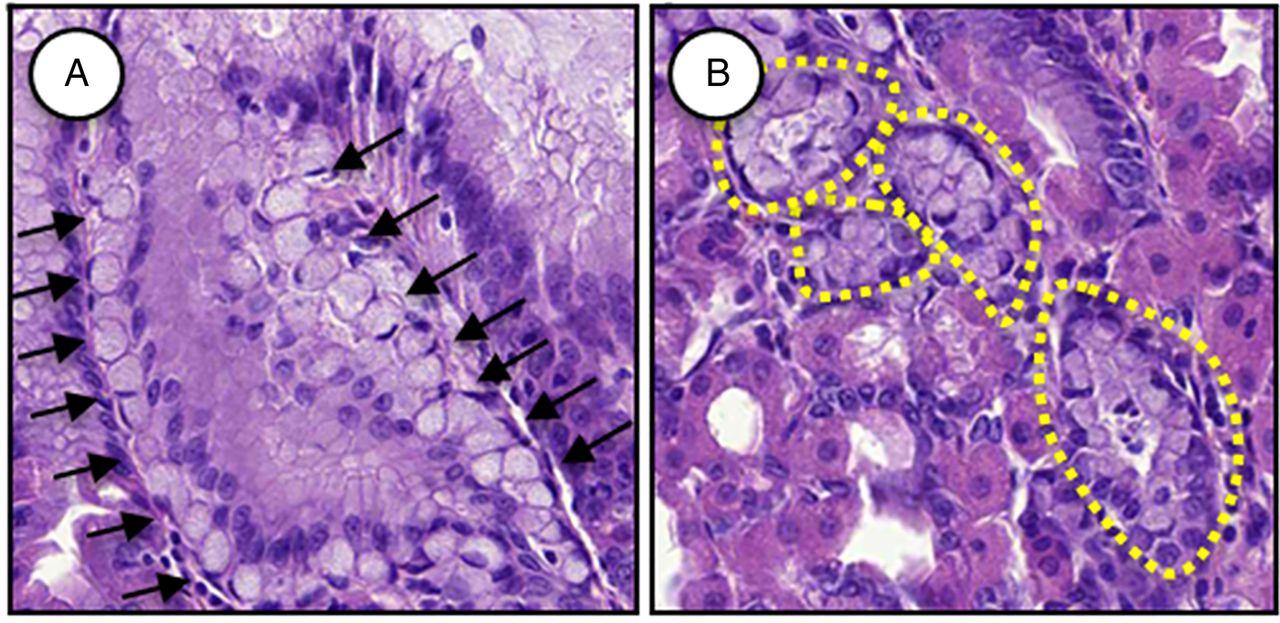
Biopsies of individuals with a family history of DGC that are endoscopically screened by the Cambridge protocol should be examined thoroughly. The biopsies should be stained for H&E at three levels and periodic acid–Schiff-diastase (PAS-D) as standard. All lesions should be recorded. Biopsies from potential carriers of a CDH1 mutation need careful evaluation by a pathologist with experience in the pathology of HDGC. In mutation carriers, the detection of specific lesions may support a decision towards prophylactic gastrectomy. In individuals without known gene defects, the detection of such lesions may be used as an additional argument that the patient is at high risk of developing cancer and that a prophylactic gastrectomy should be discussed. The specific lesions in HDGC are tiny foci of typical signet ring cells sometimes admixed with a low number of smaller atypical cells in the lamina propria without infiltration beneath the muscularis mucosa (see figure 3A–D). The two preinvasive lesions of SRCC are (1) in situ SRCC, corresponding to the presence of signet ring cells with hyperchromatic and depolarised nuclei within the basal membrane of a gland replacing the normal cells of the gland; and (2) pagetoid spread of a row of signet ring cells below the preserved epithelium of glands and foveolae, and also within the basal membrane (see figure 4A, B).84

Mucosal signet ring cell carcinoma (pT1a) H&E (A), periodic acid–Schiff-diastase (B), E-cadherin (C) and cytokeratin staining (D) (original magnifications ×200).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Precursor signet ring cell lesions: pagetoid spreading of signet ring cells (A) and in situ signet ring cell carcinoma (B) (H&E, original magnifications ×400).
Criteria for the identification of signet ring cell lesions should be strictly followed in order to diminish the risk of overdiagnosing non-specific changes and to distinguish them from lesions that mimic SRCC or precursor lesions. In the gastrointestinal tract, various benign ‘signet cell-like changes’ may mimic SRCC (see online supplementary figure S1).85–88 Therefore, confirmation of focal signet ring cell lesions in the stomach by a histopathologist with experience in this area is strongly recommended.
Histopathology of prophylactic gastrectomy: classification of microscopic foci and determination of significance
Macroscopic examination and sampling of prophylactic gastrectomies should follow specific protocols that can be found in online supplementary protocol 2. The histological examination should be made using a checklist, focusing on the items listed in table 1.
Checklist for reporting of prophylactic gastrectomy specimens
Nearly all gastrectomies (data from >100 PTG cases published) exhibit tiny mucosal foci of SRCC or in situ signet ring cells, although sometimes these were only discovered after careful review by a pathologist with experience in this field.25 ,36 ,39 ,59–64 ,77 ,91 ,92 There are numerous T1a carcinoma foci but only a low number of in situ carcinoma lesions, suggesting that invasion of the lamina propria by signet ring cells may occur without a morphologically detectable in situ carcinoma.63 ,93 It is essential that the location of biopsies within gastrectomy specimens is specifically reported to learn more about the distribution of early HDGC in the stomach.
Surgical margin status must confirm that there is no residual gastric mucosa and tumour at the margins. However, oesophageal cardiac-type glands (presumably normal constituents) are diffusely scattered in the lamina propria through all levels of the oesophagus. The risk to develop SRCC in these glands is unknown but has not been reported.94 Also, metaplastic and heterotopic gastric mucosa can be seen elsewhere in the gastrointestinal tract. In a prophylactic gastrectomy series of 19 patients, three cases (16%) showed heterotopic gastric mucosa in the duodenum, and mucosal SRCC was observed in one of them (RT van der Kaaij et al, unpublished data, 2014).
Background changes in the gastric mucosa of prophylactic gastrectomy specimens encompass mild chronic gastritis, sometimes displaying the features of lymphocytic gastritis. Foveolar hyperplasia and tufting of surface epithelium, focally with globoid change, is also a frequent finding and, in some areas, vacuolisation of surface epithelium is very striking; however, this does not seem to be a specific finding.28 ,36 ,63 ,93 Intestinal metaplasia and H. pylori infection are absent in most prophylactic gastrectomies described to date.
Histopathology: advanced HDGC
Like sporadic DGC, advanced HDGC predominantly presents as linitis plastica with diffuse infiltration of the gastric wall. Histology can show mainly or exclusively signet ring cells; however, more often these tumours are composed of a pleomorphic neoplastic infiltrate with a small subset of or without classic signet ring cells (poorly cohesive carcinoma). In a minority of cases, tumour cells are arranged in small aggregates, sometimes rosettes or glandular-like structures. A component of extracellular mucin may also be present, in which the neoplastic cells float. Although there are no specific morphological characteristics indicating the hereditary nature of the tumour, in situ lesions and pagetoid spread of signet ring cells in the surrounding normal mucosa are important clues to the diagnosis.
Review of gastric specimens of 103 HDGC families without germline CDH1 mutations showed a similar morphology compared with the advanced germline CDH1 mutation-related carcinomas (van der Post et al, unpublished data, 2014). Typical in situ lesions or pagetoid spread of signet ring cells, however, were not detected in these patients.
Histopathology: LBC
The association of LBC and germline CDH1 mutations was first reported by Keller et al.95 Large series of the histopathological findings in (prophylactic) mastectomies of CDH1 mutation carriers are not reported. Kluijt et al36 described bilateral widespread foci of lobular carcinoma in situ in prophylactic mastectomies of two female patients with germline CDH1 mutations. There are no unique histopathological findings reported in (prophylactic) mastectomy specimens that can be used to distinguish these (pre-)malignancies from sporadic LBCs. However, only few patients opt for prophylactic mastectomy and these mastectomy specimens are generally not fully embedded and examined.
Use of immunohistochemical stains
Widely invasive DGC may be easily detected on H&E sections. The use of histochemical stains for neutral mucins, such as PAS-D, is useful for the detection or confirmation of tiny intramucosal carcinomas in which the neoplastic cells are dispersed among preserved foveolae and glands. This should be performed routinely in the examination of gastric biopsies taken during endoscopy and in gastrectomies from patients with HDGC.96 A cytokeratin stain can help to confirm the epithelial nature of the signet ring cells if there is any doubt. E-cadherin immunoexpression can be reduced or absent in early gastric carcinomas, contrasting with the normal membranous E-cadherin expression in adjacent non-neoplastic mucosa.39 ,40 ,97 In pagetoid spread and in situ carcinomas, E-cadherin immunoexpression can also be reduced or absent.63 However, E-cadherin expression is not always reduced or absent; this depends on the mutation type and specific mechanisms of inactivation of the wild-type allele.40 In DGC of patients without germline CDH1 mutations, the expression pattern of E-cadherin is also often reduced or absent. Therefore, E-cadherin staining should not be used as a pre-screening method to select patients eligible for germline CDH1 mutation analysis.
In patients that present with both LBC and DGC, either synchronously or metachronously, a metastasis should be considered. Two primary tumours may be indicative for a hereditary background, but this is not always the underlying reason. Metastases from these tumours are often morphologically indistinguishable.98 Breast-associated immunomarkers are ER, BRST-2 and/or mammaglobin, while CK20 and HNF4A are suggestive for GC.99 ,100
Centres of excellence for pathological diagnosis
The pathology of HDGC is unique but not easy to recognise. Experience in this pathology is needed to provide high-quality diagnosis, both in biopsies and in resection specimens. In order to increase the experience of pathologists and the accuracy of the diagnosis, especially of precursor lesions of HDGC, it would be useful to build a virtual bank of the different types of lesions observed in the setting of HDGC. Furthermore, the working group agreed that the use of (scanned) slides to be submitted for evaluation by experienced pathologists in the field should be seriously considered.
It is pivotal to examine the full gastrectomy and full mastectomy specimens of CDH1 mutation carriers to determine the stage of cancer and additionally to better understand the phenotype and biology of this disease. Experience in the examination of prophylactic gastrectomies for HDGC is quite limited in most pathology departments due to the rarity of these surgical specimens. Additionally, the routine workload of most centres is incompatible with performing the detailed examination of hundreds of sections typically obtained after totally embedding these stomachs. In the event of a lack of pathologist experience in dealing with these cases, or restricted time available due to the pathologist's workload and laboratory resources, the entire formalin-fixed gastrectomy or mastectomy specimen can be send to an experienced pathology laboratory. An alternative option is to totally embed the stomach or breast, perform H&E and PAS-D stain on all blocks and send the slides and blocks to an experienced centre for specialist pathology reporting. If these alternative strategies are not feasible, and it is not possible to totally embed the gastric or breast specimen, this should be communicated to clinicians and the patient. Furthermore, in the event of not finding foci of SRCC, the gastrectomy should not be reported as negative for carcinoma, but as ‘no carcinoma found in xx% of mucosa examined’.
Future research on molecular pathogenesis
A critical question that remains unanswered is how long early lesions of HDGC can remain indolent until there is emergence of clinical disease that may be rapidly progressive and lethal. Continuing collection of data from patients who opt for endoscopic surveillance is essential to help answer this question. Also, a thorough analysis of the mechanisms responsible for the second hit inactivation of CDH1 in the very early lesions of HDGC is necessary to define strategies for chemoprevention.
The molecular background of patients with HDGC and without CDH1 mutations remains to be clarified, including any specific morphological features of GC in the setting of other hereditary cancer syndromes. Majewski et al23 reported a family with a germline CTNNA1 mutation presenting with multiple DGC cases and intramucosal signet ring cells. Immunohistochemistry of α-E-catenin showed absent staining in the signet ring cells, while tumours from 10 other HDGC pedigrees without CDH1 and CTNNA1 mutation stained positively. Two additional families have recently been described, one of which shared an immunohistochemical phenotype with loss of α-catenin and cytoplasmic rather than membranous E-cadherin.24 This finding suggests either that the pathogenicity of CTNNA1 mutations may be mediated through loss of E-cadherin function or that the cancer-initiating potential of CDH1 mutations is imparted through α-catenin-associated pathways. More research is needed to understand the role and mutation detection rate of CTNNA1 mutations.
Postsurgical care and nutrition
Postoperative care
The psychological, physiological and metabolic impact of a total gastrectomy should not be underestimated. The physical impact of a gastrectomy is difficult to predict for any individual, but there is an expectation that most patients will return to a full and active life after their operation. Reassuringly, global quality-of-life scores recover to presurgery levels at around 12 months postoperatively; however, problems with eating, abdominal pain and reduced body image persist beyond this time.101
Enhanced postgastrectomy recovery programmes are now well established. These programmes may include preoperative carbohydrate loading, preferably the avoidance of a nasogastric tube or abdominal drain, early mobilisation with good analgesia (epidural or local anaesthetic wound catheters), resume oral intake within 3–5 days and discharge from hospital within 7–10 days. In addition, patients often require considerable support during the first 12 months after surgery. Implementation of this support will depend upon the local healthcare services and the distances required for patients to attend the centre. Specialist nurses and dieticians should maintain regular contact by telephone and the use of modern video-conferencing should be encouraged. Collection of clinical data in a national registry allows patients, if they choose, to contribute to HDGC syndrome research.
There are different issues related to mastectomy (prophylactic or otherwise), a second major surgery with a significant recovery period. Mastectomy has a different impact concerning self-image, self-esteem, physical appearance and loss of feminine identity. Therefore, a team including a dietician, physiotherapist and psychologist should be available for optimal physical and socio-emotional recovery during postoperative care of both gastrectomy and mastectomy.
Nutrition
The main adjustments with regard to diet and nutrition postgastrectomy have to do with (1) maintaining weight; (2) ensuring adequate fluid, nutritional and caloric intake; and (3) behavioural modifications surrounding eating. Experienced dieticians focus on nutritional problems and strategies for maintaining weight after surgery, while patients focus on lifestyle changes. Patients are often discouraged by weight loss. The median weight loss 1 year postsurgery is 10 kg.101 This means that patients who are underweight preoperatively or who have a history of eating disorders need very careful counselling and support. Anatomical changes can make the act of eating difficult, and patients may become disappointed by these hurdles. This can further complicate weight management with the psychological burden of eating. In the early stages of recovery, intentional eating, drinking, management of symptoms and resting can quickly become draining. It is important for patients to have realistic expectations for their progress and improvement over time. Common postsurgical symptoms, risks and treatment options are listed in table 2.
Postgastrectomy symptoms and treatment options
Following a prophylactic gastrectomy, patients initially have to eat frequent small meals. Eating too much and/or too quickly will cause abdominal pain. Dumping syndrome is a group of symptoms commonly experienced as a result of altered gut anatomy following gastrectomy, caused by rapid entry of food into the small intestine at an earlier stage of digestion. This leads to a shift of fluid from the bloodstream to the small intestine to aid in digestion, and may lead to cardiovascular and abdominal symptoms. Late dumping is caused by a rapid rise and subsequent decrease in blood sugar levels by delayed insulin secretion. After gastrectomy, food moves rapidly and directly into the small intestine, where it digests faster. Also, the pancreas produces more insulin in a short time. This excessive insulin production allows for a rapid decrease in the blood sugar.107 These symptoms may be more common in the immediate postoperative period and often subside over time. Dumping syndrome can be minimised or eliminated through dietary choices and modified eating habits; adequate adjustments are unique from patient to patient. With time, however, these symptoms tend to improve.101 Other problems may include lactose intolerance, steatorrhoea, small bowel bacterial overgrowth, anastomotic strictures and postprandial fullness.108 ,109 Patients should be warned that their tolerance to alcohol will reduce after gastrectomy and that absorption of some medications can be affected.
As a result of malabsorption, patients with postgastrectomy are at risk for nutritional deficiencies. Monitoring of nutritional levels in postsurgical follow-up is essential as deficiencies increase risk for other symptoms and health concerns. All patients require lifelong vitamin B12 supplementation (either oral, subcutaneous or intramuscularly) to correct identified deficiencies, and close monitoring for conditions such as iron deficiency, anaemia, hypocalcaemia, osteoporosis and trace element deficiencies. Many dieticians recommend patients to take a daily multivitamin preparation with iron; however, it remains important to monitor iron levels since absorption will change after gastrectomy. While these are the most commonly reported symptoms, attention should be paid to any significant and prolonged changes, such as hair loss or extreme fatigue. These symptoms and changes away from the patient's baseline may be indicative of nutritional deficiencies, which may need to be identified and treated.
Patients should consult a dietician prior to surgery as an awareness of baseline nutritional status and dietary habits will benefit the patient in postsurgical nutrition, diet and weight management. While there are some basic dietary principles that apply to most patients with gastrectomy, there are no absolute rules. Each patient's recovery is unique, from food and quantity tolerances, to comfortable eating habits. Variability is observed between patients, but also for individual patients during the course of their recovery. The most notable changes occur within the first year; however, deficiencies should be carefully followed since they can also develop over years. Patients are encouraged to continue to experiment and discover what is best suited to their needs and tolerances.
Future research: nutrition postgastrectomy
Further studies are needed to elucidate the relationship in patients with postgastrectomy between diet, nutrition, drug absorption, changes in body composition and the direct impact on quality of life, both in the short term and long term.
Patient advocacy and the next steps in patient care and HDGC research
In patients’ experience, the process that HDGC families go through to find local medical care providers with experience with HDGC is frustrating. Faced with the lack of universal expertise, patients and advocacy groups have started working together to locate local care providers with expertise or facilitate connecting local care providers with experts at globally recognised multidisciplinary centres of excellence. Medical expertise in HDGC has to continue to grow, and this expertise has to be communicated within the medical community, such that support structures for patients with HDGC will become more easily accessible and established within existing medical systems.
Given the rare nature of HDGC, there is currently no singular global expertise portal for genetic counselling, psychosocial support, gastroenterology, surgery, pathology and postsurgery follow-up for HDGC families. The geography of existing expertise centres does not nearly cover broadly enough the areas where these resources are needed. With the emerging trend towards telemedicine, and the development of various patient advocacy groups, notably ‘No Stomach For Cancer’,110 ‘DeGregorio Family Foundation for Stomach and Esophageal Cancer Research’111 in the USA and ‘Stichting CDH1’112 in the Netherlands, we see the potential for collaboration between patients, medical professionals and patient advocacy groups to the end of empowering patients by directing and connecting them with the appropriate resources and expert opinions.
Acknowledgments
We are very grateful to Bert Siebers from the Department of Pathology of the Radboudumc for excellent assistance in the organisation of the consensus meeting. We kindly acknowledge Patricia Oliveira, the Bioinformatician that helped collecting the information for the CDH1 database, and the the support of the LOVD-team (Leiden University Medical Center, Leiden, the Netherlands) for setting up, maintaining and hosting the CDH1 database.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
- Data supplement 1 - Online appendix 1
- Data supplement 2 - Online appendix 2
- Data supplement 3 - Online figure
Footnotes
RSvdP and IPV are joint first authors.
Correction notice This article has been corrected since it published Online First. The order of the first two authors has been corrected.
Contributors RSvdP and IPV contributed equally. Concept and design: RSvdP, IPV, JHvK and RCF. Acquisition of data, analysis and interpretation of data, critical revision of the manuscript for important intellectual content, final approval of manuscript: all authors. Drafting of the manuscript: RSvdP, IPV, FC, PG, DH, NH, JHvK, RCF with input of all authors.
Funding The 8th (Cambridge, Vancouver, Porto, Munich, Siena, Seoul, Cambridge and Nijmegen) workshop of the International Gastric Cancer Linkage Consortium was made possible by generous sponsorship from the Royal Netherlands Academy of Arts and Sciences (KNAW), the Netherlands Organisation for Health Research and Development (ZonMW) and the European Society of Pathology.
Competing interests None.
Provenance and peer review Not commissioned; externally peer reviewed.