Article Text

Abstract
A recent report estimated the breast cancer risks in carriers of the three Ashkenazi founder mutations to be higher than previously published estimates derived from population based studies. In an attempt to confirm this, the breast and ovarian cancer risks associated with the three Ashkenazi founder mutations were estimated using families included in a previous meta-analysis of populatrion based studies. The estimated breast cancer risks for each of the founder BRCA1 and BRCA2 mutations were similar to the corresponding estimates based on all BRCA1 or BRCA2 mutations in the meta-analysis. These estimates appear to be consistent with the observed prevalence of the mutations in the Ashkenazi Jewish population.
- BRCA1/2 penetrance
- meta-analysis
- founder mutation
- Ashkenazi
Statistics from Altmetric.com
We recently reported the average risks of breast and ovarian cancer associated with BRCA1 and BRCA2 mutations, using a meta-analysis of pedigree data from 498 BRCA1 and BRCA2 mutation carriers identified through population based studies of women with breast and ovarian cancer.1 King et al2 estimated the risks to carriers in the three Ashkenazi founder mutations (BRCA1 185delAG and 5382insC, and BRCA2 6174delT) by genotyping the relatives of 104 mutation carriers. They concluded that the risks are higher than both our estimates or other previously published estimates.3–6 To provide a more direct comparison between the two studies, we estimated the breast and ovarian cancer risks associated with the three Ashkenazi founder mutations using families included in our meta-analysis.
Among the index cases studied by Antoniou et al,1 75 were BRCA1 185delAG carriers, 69 were BRCA1 5382insC carriers, and 52 were BRCA2 6174delT carriers. Sixty three (84%) of the 185delAG mutation carriers and 42 (81%) of the 6174delT mutation carriers were identified through studies of Ashkenazi Jewish populations. However, only 22 (32%) of the 5382insC carriers were identified through such studies, while 34 carriers (49%) were of eastern European origin.
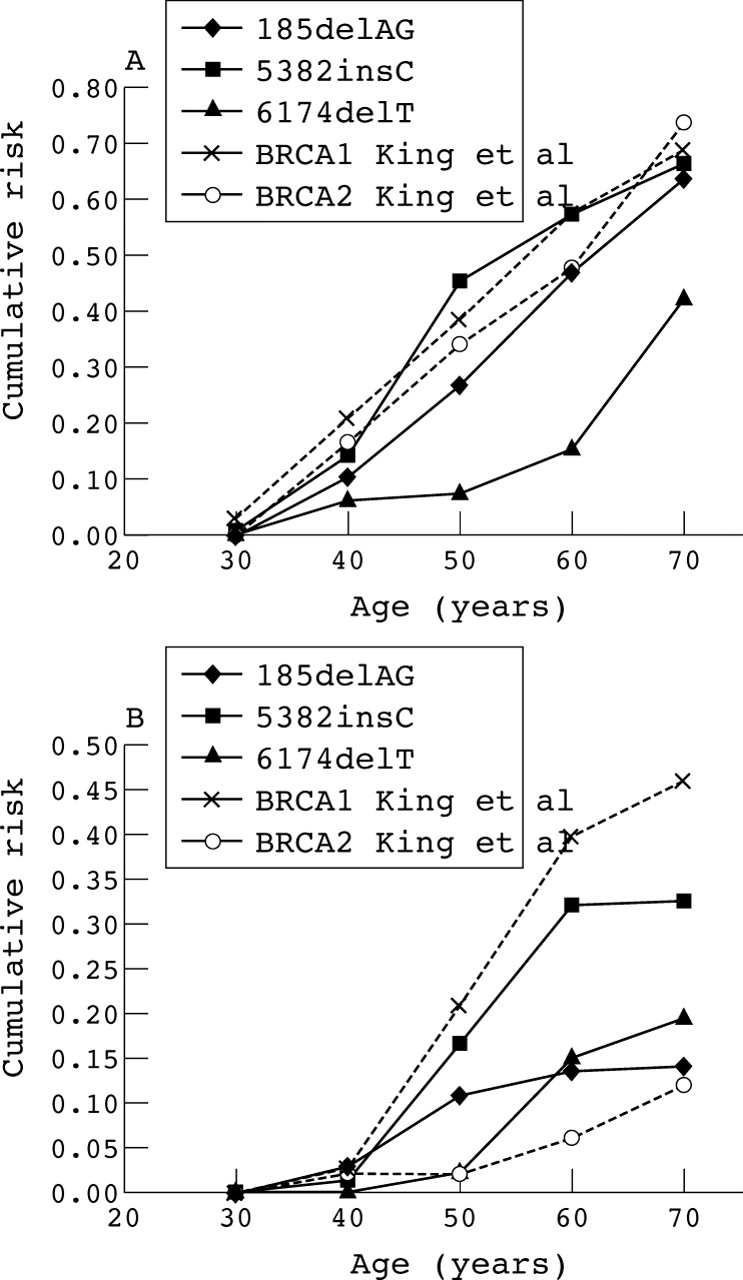
We estimated the age specific breast and ovarian cancer incidences in mutation carriers for each mutation separately using the maximum likelihood approach described in Antoniou et al.1 The estimated cumulative breast and ovarian cancer risks are shown in table 1. The breast cancer risks by age 70 were similar in carriers of the 185delAG mutation (64%; 95% confidence interval (CI), 34% to 80%) and the 5382insC mutation (67%, 95%CI, 36% to 83%) (p = 0.53 by likelihood ratio test), although the risks by age 50 were somewhat higher for 5382insC carriers (46% v 27%). The breast cancer risks for carriers of the 6174delT mutation were, however, lower (43% by age 70, 95% CI, 14% to 62%; p = 0.007 compared with all BRCA1 mutation carriers). The difference is particularly marked at age 50 (8% v 36% for BRCA1 mutations combined). The corresponding ovarian cancer risks were 14% (95% CI, 2% to 24%), 33% (8% to 50%), and 20% (2% to 35%) in carriers of the 185delAG, 5382insC and 6174delT mutations, respectively.
Estimated cumulative risks of breast and ovarian cancer in carriers of the 185delAG, 5382insC, and 6174delT mutations
Figure 1 illustrates our penetrance estimates and those obtained by King et al.2 The estimated breast cancer risks in BRCA1 mutation carriers are similar in the two studies (67% by age 70 from our study, for 185delAG and 5382insC combined, compared with 69% obtained by King et al2). However, there was a substantial difference in the breast cancer risk in BRCA2 6174delT mutation carriers (43% v 74%; p = 0.016). The 95% confidence intervals for the estimated breast cancer cumulative risks in BRCA2 mutation carriers exclude the corresponding point estimates of King et al2 at all ages. Our lower estimate is more consistent with estimates obtained by other studies.4,5 The difference in risks between BRCA1 and BRCA2 carriers also appears more consistent with the observed prevalence of the founder mutations among breast cancer cases in the Ashkenazi Jewish population.7
{kind=link}
Estimated cumulative risks of breast and ovarian cancer (A and B, respectively) in carriers of the 185delAG and 5382insC BRCA1 and 6174delT BRCA2 mutations. The estimates of King et al2 are also included.
Our estimated breast cancer risks for the Ashkenazi founder mutations were similar to the estimates obtained from our meta-analysis of population based studies for all BRCA1 and BRCA2 mutations combined.1 The ovarian cancer risks in 6174delT carriers were somewhat higher than the average BRCA2 risks (20% v 11%), consistent with the observation that mutations within the ovarian cancer cluster region are associated with a higher ovarian cancer risk.8 The ovarian cancer risk in carriers of the 185delAG mutation is lower than expected, but the confidence limits are wide. Moreover, the risks conferred by this mutation are not significantly different from the risks conferred by 5382insC (p = 0.53). Given the much larger number of families studied, the overall estimates of Antoniou et al1 probably provide a more reliable basis for risk assessment for carriers of BRCA1 and BRCA2 mutations identified through population studies than estimates based on individual mutations.
Acknowledgments
These analyses were supported by Cancer Research UK (formerly Cancer Research Campaign) and National Institutes of Health (NIH) grant 1R01 CA81203. DFE is a principal research fellow of Cancer Research UK, and PDPP is a senior clinical research fellow of Cancer Research UK. Individual studies were supported by NIH grant 1R01 CA63682, the Italian Association and Foundation for Cancer Research, the Swedish Cancer Society, European Community grant QLRI-CT-1999–00063, Hungarian Research Grants from the Ministry of Education Szechenyi Project NKFP1/48/2001 and OTKA T030039, the Icelandic Cancer Society and the University of Iceland Research Fund, and the Wessex Cancer Trust. We also thank the Department of Pathology, University Hospital Iceland; the Nordic Cancer Union; and the Cancer Society and Cancer Registry of Finland.
Footnotes
-
↵* The first two authors contributed equally to this work.
-
Competing interests: none declared