Article Text

Statistics from Altmetric.com
Williams-Beuren syndrome (WBS, MIM 194050) is a rare condition, with striking physical and behavioural features,1–3 which occurs in 1/20 000-1/50 000 live births. Cases are generally sporadic; however, familial cases with an autosomal dominant mode of inheritance have been reported. It results in a complex phenotype with physical, cognitive, and behavioural aspects that include an uneven cognitive profile (WBSCP), with verbal tasks outstripping spatial tasks, and overall IQs in the 50-60 range. Physically, WBS phenotypes include a dysmorphic face, congenital heart disease (typically supravalvular aortic stenosis (SVAS)), growth retardation, hyperacusis, premature ageing, and often infantile hypercalcaemia. These features are caused by deletion of the Williams-Beuren syndrome critical region (WBSCR) at chromosomal position 7q11.23 on either the maternal or paternal chromosome 7. The deletion is thought to arise from recombination between misaligned repeat sequences flanking the WBSCR during meiosis. The breakpoints cluster within these repeat regions, so that most WBS patients have similar deletions of approximately 1.5 Mb. A few WBS patients have, however, been reported with smaller deletions (<1 Mb).3,4 Patients with partial deletions of the WBSCR (that include the elastin gene) and SVAS as the only resulting phenotype have also been described.5 No credible cases of WBS without the deletion have so far been reported, suggesting that haploinsufficiency for a single gene will not explain the phenotype. Nineteen genes have so far been described in the WBSCR, yet only elastin hemizygosity has been confidently associated with any aspect of the WBS phenotype, namely SVAS, hernias, and possibly premature ageing. It would therefore appear that, alone or in combination, some of the remaining genes in the deleted region are responsible for the other features of WBS.
Relations between genotype and phenotype in WBS are mainly studied at the group level with rather gross measures of behavioural outcome. Yet, much is to be gained by more in depth cognitive studies. In our earlier work,5 we identified some SVAS patients who were deleted for both elastin (ELN) and LIMK1 genes, and our findings confirmed that hemizygosity for ELN causes SVAS and some of the connective tissue phenotypes (for example, hernias). The role of LIMK1 in WBS is more ambiguous. LIMK1 encodes a cytoplasmic protein kinase, expressed at high level in neurones, that phosphorylates cofilin (an actin depolymerising factor) and regulates actin cytoskeletal reorganisation.6,7 Since defects in actin turnover could affect axonal guidance during development of the central nervous system, LIMK1 is a good candidate for the mental aspects of the WBS phenotype, and LIMK1 hemizygosity has been implicated in impaired visuospatial constructive cognition.8 However, psychometric testing of our SVAS patients with small deletions encompassing the LIMK1 gene showed no evidence of the WBSCP.5
In this paper, we take Williams-Beuren syndrome as a model for cognitive profiling and examine two cases in some detail at the physical, cognitive, and molecular level. We compare the profile of one unusually high functioning patient with WBS to one SVAS patient who has a large deletion within the WBSCR. Somatic cell hybrids containing the deleted chromosome 7 were used to assess the extent of the deletions in these patients, so that genotype comparisons could be made. Analysis of such cases highlights typical differences in cognitive profiles between normal controls and all patients with WBS, whatever their intellectual level.
Key points
-
We have identified an unusually high functioning WBS patient and compared her at physical, cognitive, and molecular levels to an SVAS patient with a smaller deletion in the WBS critical region.
-
The WBS patient had a typical deletion but very high verbal scores alongside poorer spatial and non-verbal reasoning scores typical of WBS. The SVAS patient had normal development, above average cognitive profile, and no indication of spatial impairment. SVAS was the only WBS feature despite deletion of ∼60% of the WBSCR (including LIMK1).
-
Haploinsufficiency of LIMK1 cannot alone contribute to WBS spatial impairments; facial dysmorphology and cognitive impairments typical of WBS are probably caused by deletion of telomeric gene(s), either alone or acting in combination with other centromeric genes in WBSCR.
-
Comparison of these two cases highlights that even unusually high functioning WBS patients still have the characteristic chromosomal deletion and cognitive profile.
MATERIALS AND METHODS
Somatic cell hybrids
Hybrid cell lines were isolated after fusion of lymphoblastoid cells from the patients with mouse BW5147 cells as described previously.5 The presence of a single chromosome 7 in all cell lines was verified by microsatellite typing using LIMK1GT, D7S1870, and D7S669. The hybrids containing the normal and deleted chromosome 7 homologues were distinguished by PCR analysis of elastin exon 34 and LIMK1GT10 with D7S653 as a non-deleted control.
Deletion mapping of hybrids by PCR
Primers for the genes mapping to the WBSCR were designed for PCR analysis of somatic cell hybrids. Either exon 11 of the CFTR gene (CFX11) or the microsatellite marker D7S669, which map outside the deleted region, were included as internal PCR controls depending on the size of the WBS PCR products tested. Negative controls included a water blank and a mouse total genomic DNA reaction for each primer set; 50 ng of DNA, 10 pmol of each primer, and 0.5 U Taq polymerase (BCL) were used with the manufacturer’s buffer in a 20 μl reaction. PCR conditions were: two minutes denaturation at 94°C, followed by 30 cycles of 94°C for one minute, 54-65°C for one minute, 72°C for one minute, with a final five minute extension at 72°C. Primer sequences and conditions are summarised in table 1.
WSCR gene primer sequences
Cognitive-behavioural assessment
Psychometric testing was performed using the British Abilities Scales II (BAS II).11 We used six core subtests (Matrices, Quantitative Reasoning, Similarities, Word Definitions, Recall of Designs, and Pattern Construction) plus Digit Recall. For the WBS patient who is over 18 years, we used the norms for the oldest age group in the standardisation sample (17 years 6 months - 17 years 11 months). This is consistent with the procedure used in previous research.8 We also used the Peabody Picture Vocabulary Test,12 the Benton Facial Recognition Task, and the Benton Line Orientation Task,13 as well as a series of experimental tasks measuring language, memory, face processing, and number.
RESULTS
Clinical assessment of WBS and SVAS patients
Case 1 (WBS-223) is a 43 year old woman (dob 29.11.56) with Williams-Beuren syndrome who is considerably higher functioning than normally found in this syndrome. She has the typical WBS facial dysmorphology, with bilateral stellate patterns of irises and mild strabismus. Characteristic of the syndrome, she is small in stature, has a midsystolic murmur in the aortic area, suffers from hyperacusis and anxiety, and has a somewhat hoarse, monotonous voice. As a child, she suffered from hypercalcaemia and had typical hand-eye coordination difficulties. Like most patients with WBS, she is inappropriately friendly with strangers, cannot relate to peers, and in general has difficulties judging the pragmatics of social situations. She displays considerable emotional immaturity.
Case 2 (WBS-21) is a normal 11 year old girl (dob 26.6.89, aged 7 at the time of testing) who underwent surgery at 4 years of age for severe SVAS and peripheral pulmonary arterial stenosis (described in Tassabehji et al5). Mentally, she is above average. Her mother tongue is English, but at the time of examination she was attending mainstream school in France and functioning bilingually with lessons conducted in both languages. Developmental milestones are all within normal limits; she is of normal height and does not have the dysmorphic facial features of Williams-Beuren syndrome. She has no documented history of hypercalcaemia, hyperacusis, or joint problems. She displays normal interaction with adults and peers.
Case 2 was chosen for direct comparisons with case 1 in this study because: (1) she has an unusually large deletion for an SVAS patient and (2) she was perfectly matched to case 1 on verbal scores.
Molecular definition of deletions
Somatic cell hybrids were generated from lymphoblastoid cells from these two patients whereby the normal and deleted chromosome 7 homologues were separated for deletion mapping studies (two different deleted chromosome 7 hybrids were obtained and tested for each patient). Hybrids containing the deleted chromosome 7 were tested by PCR amplification for the presence of the genes spanning the region between FKBP6 and NCF1 (table 1) within the WBS critical region. Primers specific for the genes FKBP6, GTF2I, and NCF1, which map to the duplicons flanking the WBS deletion breakpoints, were designed to encompass base changes (single nucleotide polymorphisms) specific to the duplicon under investigation. The markers CF exon 11 and D7S669, mapping outside the deleted region, were included as positive controls in the PCR reactions. Mouse DNA was also included as a control to show that the PCR amplification products were human specific.
Preliminary molecular analysis of case 2 has been previously reported.5 However, since that time extensive mapping efforts have defined new genes in the region which have been included in our continuing fine mapping of the deletion status of this and other SVAS patients. The results (fig 1) show that case 2 has a large deletion (approximately 850 kb) encompassing 14 of the defined WBS genes including the whole of the WBS critical region proximal to ELN. Despite her high functioning, case 1 with Williams-Beuren syndrome has a typical WBS deletion. This includes 18 of the described genes in the WBSCR (we confirmed deletion of FKBP6, BCL7B, STX1A, ELN, LIMK1, WBSCR1 (E1F4H), WBSCR5 (WBSCR15), RFC2, CYLN2, GTF2IRD1, and GTF2I; the remainder of the 18 genes lie between pairs of deleted genes) and part of NCF1 (exon 2 is deleted but not exon 6). The deletion spans a genomic region of approximately 1.4 Mb (fig 1).

Deletion mapping of cases 1 and 2. Diagram showing a map of the WBSCR and genes deleted in the patients (diagram not to scale). PCR analysis of somatic cell hybrids from the deleted chromosome 7 homologues of cases 1 and 2. Panel A: case 2; B: case 1; C: normal control. Control primers were included in the reactions as internal non-deleted controls; CFX11 (top band) in lanes 1-9, 11-13, 16, 17, and D7S669 (bottom band) in lanes 10, 14, 15). Case 2 is deleted from FKBP6 to RFC2; case 1 is deleted from FKBP6 to part of NCF1.
Cognitive profile of case 2
In response to evidence from a study suggesting that LIMK1 haploinsufficiency contributes to the spatial impairment in WBS,8 we carried out cognitive profiling of four SVAS patients all with deletions of at least ELN and LIMK1 and found no evidence in any of them of the linguistic/spatial imbalance typical of patients with WBS.5 There was no facial dysmorphology in any of these SVAS patients. More recent inspection of photographs of two of the SVAS patients at different periods in infancy, childhood, and adolescence through to adulthood (data not shown) showed no facial features reminiscent of the facial dysmorphology typical of WBS. This excludes a contribution of ELN alone to this latter phenotype.
Case 2, the patient with the largest deletion, was the highest functioning of these four SVAS patients, displaying an above average, even cognitive profile, with no indication of a spatial impairment.5 This is evident from her scores on the British Abilities Scales II (BAS II). BAS II standard scores have a mean of 100 and a standard deviation of 15. Average scores for a typically developing child are therefore around 100 (classification labels and centiles for BAS II verbal, non-verbal reasoning, and spatial scores are shown in table 2). Case 2 had a verbal standard score of 110, a non-verbal reasoning score of 118, and a spatial score of 115. In particular, she scored above average on the Pattern Construction subtest of the BAS II, while scores of WBS patients are typically at floor (that is, the lowest possible level) on this test. This highlights the fact that haploinsufficiency of LIMK1 alone cannot contribute to the WBS spatial impairments since, like all WBS patients described to date, Case 2 is hemizygous for this gene.
Descriptive classification labels and centiles for BAS II verbal, non-verbal reasoning, and spatial score
Cognitive profile of case 1
Over the past 10 years we have carried out in depth cognitive profiling of over 100 WBS patients ranging from age 9 months to 53 years.14–17 Case 1 is the highest functioning patient tested to date. On the Wechsler Adult Intelligence Scale, she had a full scale IQ of 93 and a verbal IQ of 99 (both close to the average score in the normal population of 100) and a performance IQ of 86 (at the lower end of the normal range). Although these measures do not bring out very strikingly the discrepancy between her verbal and spatial scores, other tests do highlight the typical pattern of her WBS profile. On the British Abilities Scale II, she had an impressive verbal standard score of 112, but a non-verbal reasoning score of 64 and a spatial score of 55, typical of the low levels seen in patients with WBS (see table 2 for classification of BAS II scores). Her verbal score was significantly higher than any WBS patient we have tested, as was her score on the Peabody Picture Vocabulary Test (standard score of 107 where the average is 100). On language specific experimental tasks, case 1 scored almost at ceiling (that is, the highest possible level), compared with other WBS patients who score around the equivalent of their mental age, albeit always better than their spatial performances. The inspection time of case 1 (amount of time required to inspect a display to make a decision) was significantly longer than normal controls, but shorter than the majority of people with WBS. All experimental tasks of verbal memory showed high scores in this patient, much higher than in other WBS patients. On the Benton Facial Recognition task she scored within the normal range, typical of many people with WBS. However, like most people with WBS she scored at floor on the Benton Line Orientation Task, attesting once more to her spatial problems.
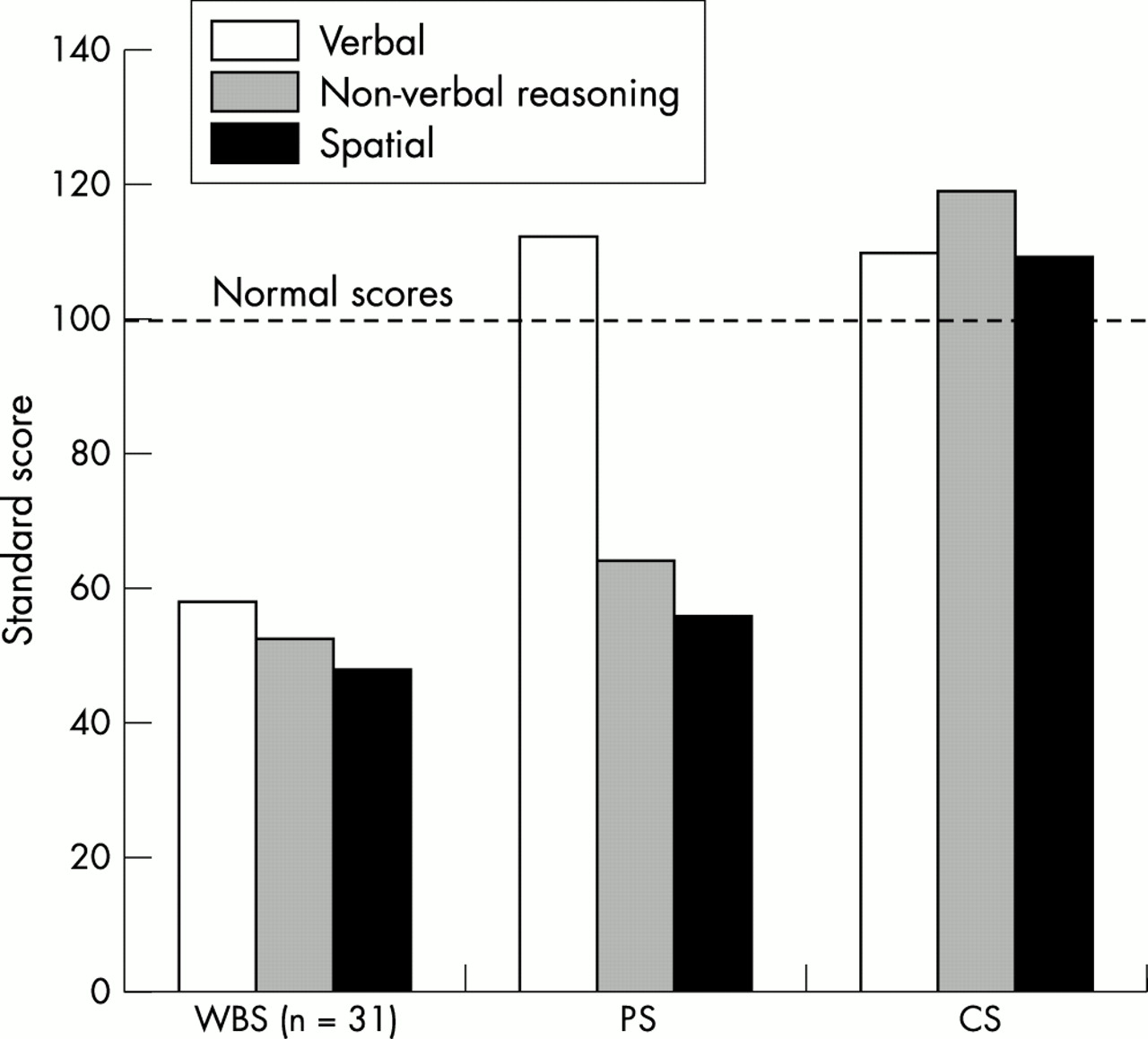
Fig 2 shows how, notwithstanding the possibility of clearly matching these two patients on their verbal scores, the patterns of their cognitive profiles differed significantly. Despite above average scores for the syndrome, case 1 resembled the typical uneven profile of Williams-Beuren syndrome. In contrast, the SVAS patient (case 2) displayed an even profile across both language and spatial measures.
{kind=link}
{kind=link}
Comparison on British Abilities Scale-II of typical WBS patients (WBS), case 1 (PS), and case 2 (CS) on verbal (SD 10.29), non-verbal reasoning (SD 5.87), and spatial scores (SD 2.19). The dotted line represents normal control scores.
DISCUSSION
Unravelling the relationship between genes and the cognitive/behavioural components of Williams-Beuren syndrome is a complex task. We have approached this by carrying out detailed cognitive assessments on a large number of subjects with WBS, to identify those with a somewhat different cognitive profile from the classical cases. These have been compared with subjects who have partial deletions in the same region that have resulted in only single, non-cognitive features of Williams-Beuren syndrome, SVAS in the present case. Since the uneven profile is a near universal feature of Williams-Beuren syndrome and the 7q11.23 deletion is the only genetic factor common to all WBS patients, it is reasonable to assume that the determinants of the WBS cognitive profile map within the WBS critical region.
Comparing the two cases reported here, they have similar high verbal test scores and have many of the same genes deleted, yet case 1 has the typical WBS cognitive profile, while case 2 does not, high scores of case 2 were evenly distributed across verbal and spatial tasks, whereas in case 1, although verbal scores were as high as those of case 2, spatial scores (and non-verbal reasoning scores) were very poor and typical of WBS. The comparison suggests that the features of WBS apart from SVAS are caused by deletion of genes in the CYLN2 - NCF1 region at the telomeric end of the WBS critical region.
It has been suggested18 that case 2 might be mosaic, so that the deletion is not present in the cells of her CNS. This suggestion is impossible to disprove, since her deletion, as in virtually all WBS patients, is de novo, and no laboratory test can ever totally exclude mosaicism in somebody with a de novo change. We think the suggestion is implausible for three reasons. First, mosaicism would most likely arise by mitotic recombination, which occurs at approximately 10-4 times the frequency of the meiotic recombination that produces the typical WBS deletions. Second, the deletion is present in both her lymphocytes and vessel walls, which would imply a very early embryonic origin of the deletion. Finally, case 2 is not our only patient with a LIMK1 deletion but no WBS cognitive profile; we have previously described two others.5 Thus, we doubt that case 2 is a mosaic, and together with our previously described cases, we think that she shows that deletion of LIMK1 does not of itself produce the WBS cognitive profile. It remains possible that the profile results from deletion of LIMK1 together with deletion of one or more of the genes from the part of the WBS critical region that is not deleted in case 2.
Our genotyping results do not explain why case 1 is so high functioning: her deletion is not clearly different from those in typical WBS patients. One plausible explanation is the contribution made by her parents. They have well above average IQs, as do her sibs. Therefore her verbal score of 112 could be the result of her high biological potential and thus still involve a typical WBS deficit. However, detailed characterisation of her telomeric breakpoint might indicate a genetic cause; our findings suggest that genes at the telomeric end of the WBS deletion are likely to be important in causing the WBS cognitive profile.
Further studies require the identification and in depth cognitive profiling of other subjects with different sized deletions in the WBSCR. Detailed molecular and clinical characterisation of subjects with variations on the classical WBS phenotypes or classical WBS deletions are important tools for dissecting the roles of each of the genes, within the WBS critical region, in the different aspects of this fascinating developmental disorder.
Acknowledgments
We are grateful to the patients involved in the study for their cooperation. MT was supported by the Wellcome Trust (grant No 061183). AK-S was supported by MRC Programme Grant No G9715642. MC was supported by The Birth Defects Foundation.