Article Text

Statistics from Altmetric.com
Autosomal dominant optic atrophy (ADOA) is the most common form of autosomally inherited optic neuropathy, with an estimated prevalence of 1:50 000 in most populations,1 though it can reach 1:10 000 in Denmark.2 The disease typically presents in childhood with variable bilateral slow visual loss, temporal optic nerve pallor, centro-caecal visual field scotoma, and abnormalities of colour vision.3 In most families, the disease is accounted for by mutations in the OPA1 gene, at the OPA1 locus on chromosome 3q28–q29 (MIM165500). The penetrance of the OPA1 disease is highly variable as well as its age of onset, even within the same family.
Some ADOA families have been shown to exclude linkage to the OPA1 locus.4,5 In 1999, the genetic study of a large family whose phenotype was similar to the OPA1 phenotype, allowed the mapping of a second ADOA locus on chromosome 18q12.2–q12.3 (OPA4, MIM605293).5 To date, no report has confirmed this localisation and the disease gene is still unknown.
Here we report the mapping of a third ADOA locus on chromosome 22q12.1–q13.1 (OPA5) in two unrelated families affected with a OPA1-like phenotype.
METHODS
Patients
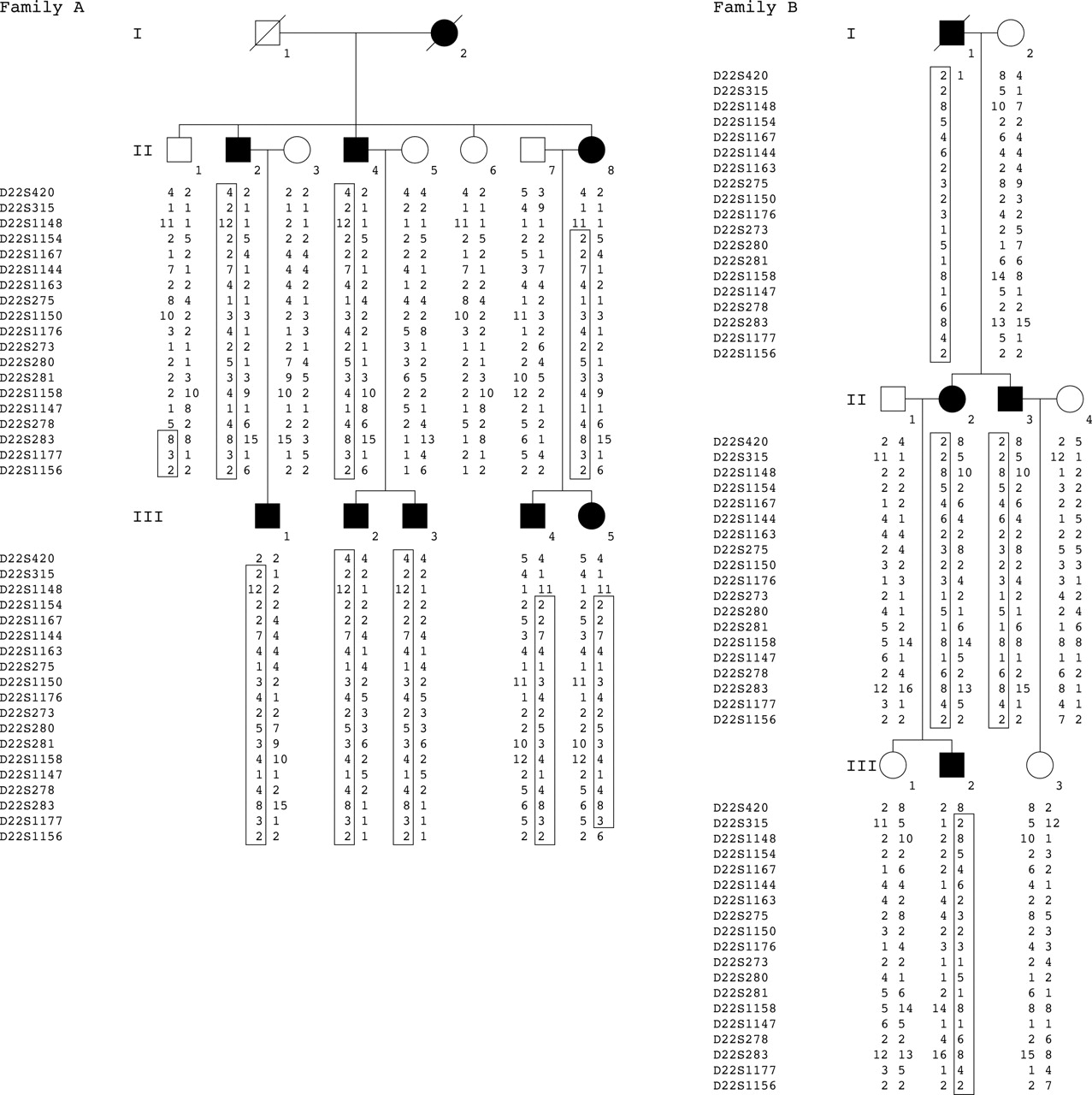
Two unrelated multiplex families of French origin affected with autosomal dominant optic atrophy were ascertained through the genetic consultation clinic of the Hôpital des Enfants Malades in Paris (family A and family B; fig 1 A and B, respectively). All members of each family underwent ophthalmological examination including visual acuity measurements, visual field testing, colour vision analysis, ocular pressure measurement, examination of the fundi, and electrophysiological recordings. Blood was collected from all family members and the DNA was purified by phenol-chloroform extraction.

{kind=link}
Haplotype of families A and B at the OPA5 locus on chromosome 22q12.1–q13.1, respectively. The disease haplotype is squared in each patient.
Linkage analysis
Linkage to known ADOA loci was studied in both families. Four markers flanking the OPA1 locus on chromosome 3q28–q29 were chosen from the Généthon linkage map on the basis of their informativeness6—AFM308yf1, AFMa300wa5, AFMb043xe9, and AFM254ve1 at the D3S1601, D3S3590, D3S2748, and D3S1311 loci, respectively. For the OPA4 locus, we selected three markers lying in the genetic interval on chromosome 18q12.2–q12.3 as well as two flanking markers: AFM147yf2, AFM191vc7, and AFM284ve1 at the D18S1094, D18S450, and D18S472 loci, respectively; and AFMa224wb1 and AFM295xh1 at the D18S1102 and D18S474 loci.
A 10 cM genome-wide search for the disease causing gene was undertaken in family A using fluorescent oligonucleotides flanking the 382 polymorphic markers of the Genescan Linkage Mapping Set, version II (Perkin Elmer Cetus), under conditions recommended by the manufacturer. Amplified fragments were electrophoresed and analysed on an automatic sequencer (ABI 3100, Applied Biosystems, Foster City, California, USA). Linkage analyses were carried out using M-LINK and LINKMAP of the 5.1 version of the Linkage program.7,8 All allele frequencies were available from the CEPH database. The gene frequency was estimated to be 1/1000 and the penetrance of the disease to be 100%.
Key points
-
Autosomal dominant optic atrophies (ADOA) are by far the most common mendelian cause of primary hereditary optic neuropathy. A major locus has been mapped to chromosome 3q28–q29 and the OPA1 gene identified. The penetrance of the disease accounted for by mutations in this gene is reported to be highly variable. A second locus, OPA4, has been mapped on chromosome 18q12.2–q12.3 in a family whose phenotype was similar to that of OPA1 patients.
-
We report the mapping of a third locus of ADOA, OPA5, on chromosome 22q12.1–q13.1 in two unrelated families of French origin. The phenotype of affected patients of the two families was similar to that of patients harbouring OPA1 mutations.
-
The OPA5 locus lies in a 10.4 Mb interval flanked by the D22S1148 and D22S283 loci. To date, 73 known genes and as many predicted genes are contained in this interval. Screening of OSBP2, C22ORF3, HSC20 and HSPC051 failed to identify any mutation.
Screening for mutations in candidate genes
The 14 exons encoding the oxysterol binding protein 2 (OSBP2), the five hypothetical exons of the chromosome 22 open reading frame 3 (C22ORF3), the six exons of the J type co-chaperone HSC20 gene, and the two exons of the ubiquinol-cytochrome c reductase 7.2 kDa complex (HSPC051) were amplified using specific primers designed from intronic sequences close to the intron-exon junctions (not shown, available on request). Amplified products were purified by phenol-chloroform extraction, recovered by ethanol precipitation, and directly sequenced using the Big Dye terminator cycle sequencing kit V3 on a 3100 automated sequencer (ABI Prism, Applied Biosystems).
RESULTS
Clinical evaluation
We report two unrelated multiplex families of French origin affected with ADOA. Although the age of onset of the disease differed (in the first and the third decades), the phenotype was similar in both families. When examined, the fundus of patients constantly showed optic nerve pallor. Visual acuity decreased slowly, perhaps related to a central scotoma. Colour vision was moderately impaired, varying from normal to blue-yellow dyschromatopsia. After several years of evolution, the patients show a severe dyschromatopsia without axis. Electroretinogram recordings were normal while visual evoked potential recordings were moderately altered in the early stages and severely impaired in the later stages. In both families, the phenotype of affected patients was similar to that of patients harbouring mutations in the OPA1 gene.
Exclusion of the OPA1 and OPA4 loci
Linkage studies at the OPA1 and OPA4 loci allowed the exclusion of the two loci in both families (not shown, available on request).
Mapping of a third locus for ADOA (OPA5)
A genome-wide search was undertaken to map the disease gene in family A. All eight affected patients were found to share a common haplotype on chromosome 22q12.1–q13.1 (family A, fig 1A). Obligatory recombination events in the affected individual (II8) and her healthy brother (I1) allowed us to define a 10.4 cM genetic interval between the D22S1148 and D22S283 loci (family A, fig 1).
Linkage to the 22q12.1–q13.1 ADOA locus was sought in family B. Interestingly, all affected patients of this family were found to harbour the same haplotype, inherited from the affected grandfather I2 (family B, fig 1B). No recombination event was found with the markers of the region.
When the two families were taken into account, a maximum lod score of Zmax = 3.75 at h = 0 was obtained with the marker AFMa043tf9 at the D22S1176 locus (table 1). For this calculation, the penetrance was set at 100% (12 of 12 individuals with a disease haplotype were affected with ADOA).
Two point lod score values for the two families between the disease and the markers of the 22q12.1–q13.1 chromosomal region (OPA5)
Candidate genes study
Three know genes—OSBP2, HSC20, and HSPC051—which encode the oxysterol binding protein 2, the J-type co-chaperone HSC20, and the ubiquinol-cytochrome c reductase 7.2 kDa complex, respectively, as well as the hypothetical chromosome 22 open reading frame 3 (C22ORF3), were screened for mutations. No disease causing alteration was found in any of the two families. Only already reported single nucleotide polymorphisms (Human Genome Project working draft at UCSC) were identified in the two families (not shown, available on request).
DISCUSSION
The primary hereditary optic neuropathies comprise a group of disorders in which there is cell death confined to the retinal ganglion cells. Dominant optic atrophies are by far the most common mendelian cause of primary hereditary optic neuropathy.9 A major locus has been mapped to chromosome 3q28–q29 and the OPA1 gene identified (MIM 165500). A second locus, OPA4, has been identified in a large family of German descent from western Maryland.5
We report here the mapping of a third locus, OPA5, on chromosome 22q12.1–q13.1, in two unrelated families of French origin, both affected with a phenotype similar to the OPA1 related phenotype.
A high variation of the penetrance of optic atrophies has been reported. With regard to OPA1, the penetrance has been shown to range from 43% to 100%.10,11 In the two families reported here, the penetrance of the disease was assumed to be complete, especially as fundal examination showed optic nerve pallor in all affected patients, even when the visual acuity was still normal and the visual field only very slightly impaired. Thus the recombination event occurring in the unaffected individual II1—whose fundus and visual field were strictly normal at 78 years of age—allowed us to define the centromeric boundary of the OPA5 genetic interval at the D22S283 locus (family A, fig 1A)
The OPA5 genetic interval defined by the D22S1148 and D22S283 loci encompasses 10.4 Mb on chromosome 22q (Human Genome Project working draft at UCSC). Seventy three known genes and as many predicted genes are reported to lie in this interval. Several of them were considered as a candidate for ADOA. The gene encoding the oxysterol binding protein 2 (OSBP2) was first considered in view of its high degree of expression in the retina where it could play an important role in mediation of oxysterol cytotoxicity.12 Screening of the 14 OSBP2 exons in both families failed to identify any mutation. Subsequently, considering that the rhomboid type protease Pcp113 is involved in the processing of the yeast ortholog of OPA1, Mgm1, we considered the hypothetical C22ORF3 gene as candidate; this is predicted to encode a protein containing a rhomboid domain (National Center for Biotechnology Information). As for OSBP2, no mutation was found in the patients of either family.
It is worth remembering that all known genes involved in hereditary optic neuropathies are either mitochondrial (LHON, MIM535000) or encode proteins with high mitochondrial targeting (OPA1; OPA3, MIM606280; TIMM8A, MIM300356; SDHA, MIM600857). Therefore the exclusion of OSBP2 and C22ORF3 prompted us to screen the genes of the OPA5 interval known to encode proteins involved in the mitochondrial function. The genes encoding the J type co-chaperone HSC20—a 235 amino acid protein involved in the mitochondrial iron-sulphur pathway14—and the ubiquinol-cytochrome c reductase 7.2 kDa complex HSPC051 were screened for mutations but no alteration was found.
Further studies are required to identify the causative ADOA gene in these two families and to delineate the role of this locus.
ELECTRONIC DATABASE INFORMATION
CEPH database, http://www.cephb.fr/test/cephdb/ (for identification of allelic frequencies).
Online Mendelian Inheritance in Man (OMIM), http://www.ncbi.nlm.nih.gov/entrez/ (for OPA1 [MIM 165500, 605290], OPA4 [MIM 605293], OPA3 [MIM 606280], LHON [MIM 535000], SDHA [MIM60085], TIMM8A [MIM 300356]).
UCSC Human Genome Project working draft, http://genome.ucsc.edu (for marker order and genetic distance between markers).
National Center for Biotechnology Information, http://www.ncbi.nlm.nih.gov/ (for identification of candidate genes in locus of interest).
Acknowledgments
This work was supported by the Association Retina France and the Association Valentin Haüy.
REFERENCES
Footnotes
-
Competing interests: none declared