Article Text

Statistics from Altmetric.com
The availability of MRI has greatly increased the detection of cavernous malformations of the CNS in both symptomatic and asymptomatic patients. These lesions may be responsible for previously unexplained neurological events or may even have been incorrectly diagnosed. Cavernomas have a characteristic MRI appearance consisting of an area of mixed signal intensity, thought to be due to extracellular methaemoglobin, surrounded by an area of reduced signal intensity reflecting a zone of haemosiderin. Missing an angiographically occult vascular malformation on MRI seems likely only if the lesion contains no haemoglobin breakdown products or is microscopically so small as to be unidentifiable. This may explain the sudden appearance or “growth” of cavernomas occasionally described.
{kind=link}
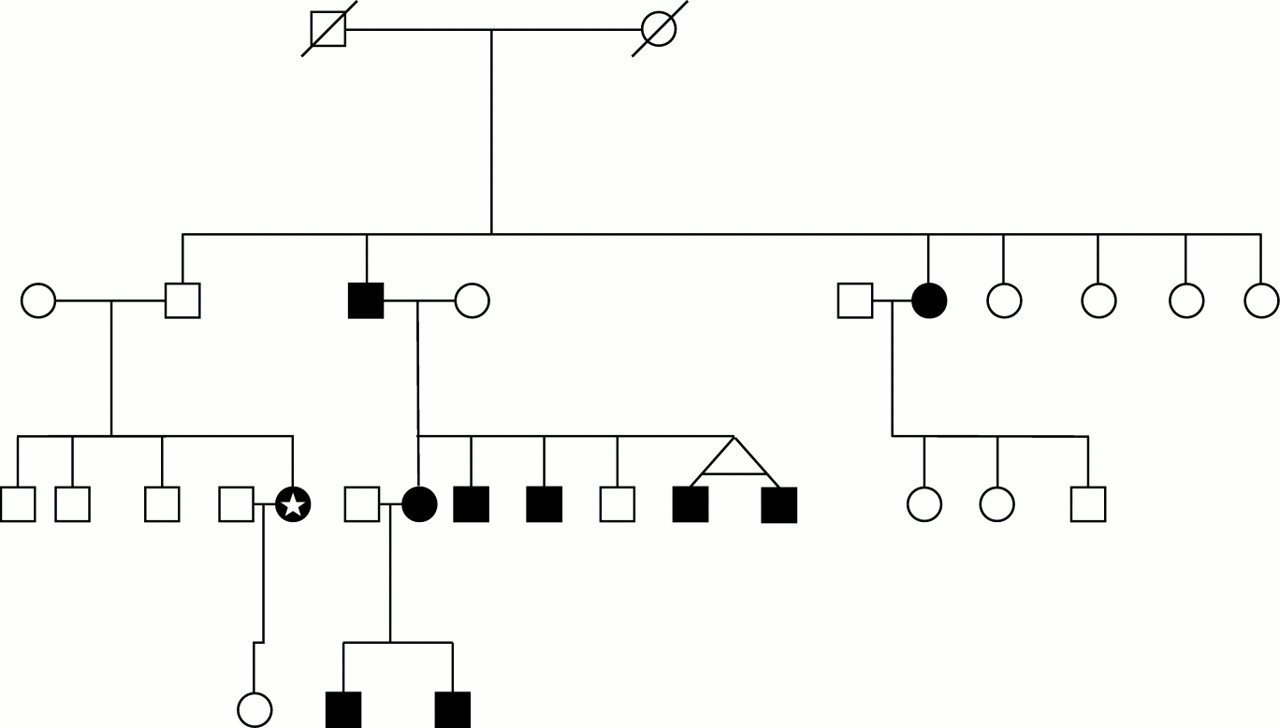
The family tree. Males appear as squares and females as circles. Affected people are shaded and those who are dead appear with an oblique slash. The original reference case is marked with an asterisk.
We report on a family, spanning three generations, in which at least 10 members are affected. The original reference patient was a woman aged 34. She developed a sudden weakness of the left leg subsequently found on MRI to be due to a rare intramedullary cavernoma at C3. Two intracranial cavernomas were also found during the same study. All three were subsequently removed. It has been suggested that in patients in whom multiple lesions are found a familial link is more likely. We therefore took a detailed family history. The patient told us of an aunt who has epilepsy. She had recently been diagnosed by CT as having a low grade glioma. Subsequent MRI studies have shown the lesion to have the characteristics of a cavernoma. As the family tree (figure) was constructed it became apparent that five first cousins—four males (two of whom are monozygotic twins) and one female, all siblings—had presented independently to different consultants at our institution with either seizures or unexplained intracerebral haemorrhages. Brain MRI studies in the males had shown multiple intracerebral cavernomas. Their sister has two epileptic children, both shown to have cerebral cavernomas. She was symptom free and declined investigation, until the development of persistent headaches. Brain MRI has now shown intracranial cavernomas. When the medical history of the siblings’ parents was reviewed, their father admitted to a sudden spontaneously resolving hemiparesis when aged 20. He was noted to have the cutaneous angiomas sometimes associated with this condition. He was anxious to undergo investigation. Brain MRI has disclosed multiple cavernomas in the brain.
The familial occurrence of cavernomas has been reported previously, notably in Mexican-American families.1 As in the family we report, it takes the form of multiple intracranial lesions. The inheritance would seem to be autosomal dominant with strong penetrance. Recently the gene implicated has been mapped to the 7q locus.2 The finding of more than one cavernoma in one person should alert investigators to the possibility that other family members may be affected.
The surgical treatment of CNS cavernomas remains controversial. It seems that most cavernomas show evidence of previous haemorrhage to varying degrees. Most surgeons would agree on surgery in a symptomatic patient with a readily accessible lesion. An argument for surgery can also be made with lesions producing repetitive or progressive symptoms where there is significant neurological disability.3Unfortunately, to date predictors of timing and size of haemorrhage are unclear. However in a recent study involving 145 patients the authors suggest that risk factors for “aggressive behaviour” include pregnancy, familial or multiple form, previous whole brain or stereotactic radiotherapy, incomplete removal, associated venous malformation, and female sex.4 A conservative approach is best adopted when a clinically silent lesion in an eloquent area is discovered incidentally or in the case of multiple clinically silent lesions. In cases of epilepsy, well controlled on drugs, many would adopt a conservative approach. Further controversy surrounds management strategies after a single bleed in a vital area such as the brain stem. Options here include MR directed stereotactic radiosurgery or direct surgery, which has been achieved with acceptable morbidity.5
Review of the literature has shown this to be the largest number of affected members in a single family