Article Text

Abstract
Gastric cancer is one of the major causes of cancer-related death worldwide. Familial clustering is observed in about 10% of cases; 1–3% of cases are hereditary. In the latter group, a syndrome which has been well characterised is hereditary diffuse gastric cancer; this is specifically associated with CDH1 (E-cadherin) germline mutations in about 30% of families. In this article, the state of the art of familial gastric cancer regarding the clinical, molecular and pathology features is reviewed, as well as the practical aspects for a correct diagnosis and clinical management.
Statistics from Altmetric.com
Gastric cancer is the second leading cause of cancer-related death worldwide. About 90% of gastric cancer cases appear in a sporadic setting, whereas familial clustering is observed in the remaining 10%.1 Of these, only 1–3% of cases are hereditary.2 In this article, we will review the molecular and pathology features of familial gastric cancer, with an emphasis on hereditary diffuse gastric cancer (HDGC), mainly focusing on practical aspects for a correct diagnosis and management.
CLINICAL CRITERIA OF FAMILIAL GASTRIC CANCER
In familial aggregation of gastric cancer, several situations can be identified: cases in which the histopathology of the tumours is unknown, and are simply designated as familial gastric cancer (FGC); and cases in which it is possible to have information on the histopathological type of one or more gastric cancers. The latter group encompasses the following specific syndromes/diseases: hereditary diffuse gastric cancer (HDGC), familial diffuse gastric cancer (FDGC) and familial intestinal gastric cancer (FIGC).
In 1999, the International Gastric Cancer Linkage Consortium (IGCLC) defined the following criteria for identification of HDGC families: (1) two or more documented cases of diffuse gastric cancer in first/second degree relatives, with at least one diagnosed before the age of 50; or (2) three or more cases of documented diffuse gastric cancer in first/second degree relatives, independently of age.3
Families with aggregation of gastric cancer and an index case with diffuse gastric cancer, but not fulfilling the IGCLC criteria for HDGC, are classified as familial diffuse gastric cancer (FDGC).
GENETIC BASIS OF HDGC
In 1998, Guilford et al described germline truncating CDH1 mutations in three Maori families with autosomal dominant diffuse gastric cancer.4 Since then, many studies have reported different types of CDH1 mutations in HDGC families; it has been calculated that approximately 30–40% of the HDGC families harbour CDH1 germline mutations as reviewed by Oliveira et al.5–7
The CDH1 gene localises in the long arm of chromosome 16, comprises 16 exons transcribed into a 4.5 Kb mRNA and encodes for E-cadherin.8 E-cadherin is a transmembrane protein that is predominantly expressed at the basolateral membrane of epithelial cells, where it exerts cell–cell adhesion and invasion suppression functions.9 The extracellular domain of E-cadherin plays a key role in the correct folding and homo- and hetero-dimerisation of the proteins, as well as in the adhesion mechanism itself. The cytoplasmic domain of the protein interacts with the catenins (α, β, γ, p120ctn), indirectly influencing the actin cytoskeleton organisation.10 11
CDH1 mutation frequency in families with HDGC and FDGC
In order to assess the real CDH1 mutation frequency in families with diffuse gastric cancer (DGC), we analysed separately case reports of one or two CDH1 positive families (listed in the lower part of table 1) and studies on screening of CDH1 germline mutations in at least three families with diffuse gastric cancer (listed in the upper part of table 1). The latter encompass 23 studies, reporting 267 families, 151 HDGC and 116 FDGC. Among the 267 families, 62 (23.2%) harboured CDH1 germline mutations, the frequency varying with family type (HDGC vs FDGC): CDH1 mutations were identified in 46/151 HDGC families (30.5%) and in 16/116 FDGC families (13.8%). Interestingly, the frequency of CDH1 germline mutations was found to be much higher in families from regions with low incidence of gastric cancer, such as North America, North Europe and New Zealand (53/198; 26.8%) than in countries with a high incidence of gastric cancer (Japan, Korea and South Europe) (9/69 families; 13.0%). In the latter, most families may well represent the aggregation of gastric cancer cases associated with environmental factors, rather than with a CDH1 germline defect.
Type of CDH1 mutations
Altogether, 68 CDH1 germline mutations were identified in 273 (24.9%) families reported to date in the literature, encompassing those described in the 23 abovementioned studies (267 families) (62 mutations; 23.2%) and those described in five reports of isolated families (6 families) (6 mutations; 100%). Among all reported CDH1 germline mutations, 53/68 (77.9%) typed as nonsense, splice-site and frameshift mutations (predicted to produce premature termination codons) and 15/68 (22.1%) as missense mutations (see table 1 for results and references). Mutations span the whole length of the gene and hot spots have not been identified in HDGC.
CDH1 IN EARLY-ONSET DIFFUSE GASTRIC CANCER
The age of onset has been used in several types of hereditary cancer syndromes to recruit patients without a family history for genetic screening, these isolated patients representing putative carriers of de novo germline mutations. Guilford et al reported the first young patient with apparently sporadic diffuse gastric cancer, carrying a CDH1 germline mutation.14 Later, the study of a series of 66 individuals with apparently sporadic gastric cancer developed before the age of 52, led to the identification of two different germline missense alterations in 3/37 (8.1%) diffuse gastric cancer patients.39 In a series of 10 diffuse gastric cancer patients younger than 35 years, Suriano et al detected pathogenic mutations in two patients (20%) and proposed that the cut-off age for screening CDH1 germline mutations in early-onset diffuse gastric cancer should be decreased to 35 years.31
CELLULAR EFFECTS OF CDH1 MISSENSE MUTATIONS
Functional in vitro assays for CDH1 missense mutations have been developed by our group39 and are currently offered to the scientific community. Briefly, cell lines stably expressing germline missense E-cadherin mutations are characterised for cell–cell adhesion, suppression of invasion and migration, using cells stably expressing wild-type E-cadherin as control. Using this in vitro approach, we demonstrated that a proportion of CDH1 germline missense mutations harbour functional consequences in vitro, including loss of cell adhesion and promotion of cell invasion.39–41
ASSESSMENT OF THE PATHOGENIC ROLE OF MISSENSE MUTATIONS
The pathogenic role of CDH1 missense mutations represents a clinical burden in genetic counselling, as pathogenic relevance of these mutations is not straightforward. Taking into account the recommendations of Fitzgerald and Caldas42 and Suriano et al,43 we consider it mandatory for the assessment of the pathogenic significance of a missense mutation to take into account the following data: (i) co-segregation of the mutation with diffuse gastric cancer (within pedigrees); (ii) mutation frequency in the healthy control population; (iii) mutation recurrence (in independent families). However, one has to be aware of the difficulty of performing segregation analyses in some pedigrees, with a small number of affected cases available for molecular diagnosis. To overcome this problem, in vitro functional analyses of missense mutations constitute an alternative approach to determining their pathogenic relevance.39–41 To have complete information on the putative functional role of these mutations, Fitzgerald and Caldas42 stressed the need to perform transcript analyses to look for activation of cryptic splice sites. Very recently, Suriano and colleagues presented a working model to identify the pathogenic significance of missense CDH1 mutations that adds, to the previous items, functional in silico mutation analysis and integrates clinical, in vitro and in silico information into a statistical model to evaluate the divergence from neutrality of a given mutation.43
SECOND-HIT INACTIVATION MECHANISM OF E-CADHERIN
Germline CDH1 mutation carriers who develop diffuse gastric cancer generally display abnormal or absent E-cadherin expression,44 45 in accordance with the two-hit model of tumour suppressor gene inactivation. The CDH1 gene can be inactivated by a number of mechanisms. Somatic mutations have been reported in tumour samples in sporadic diffuse gastric carcinomas,46 but have rarely been described as second-hit mechanisms in hereditary diffuse gastric carcinoma.47
Alternative second-hit mechanisms of CDH1 inactivation have been shown to be CDH1 promoter methylation (both in sporadic and hereditary settings of diffuse gastric cancer)47 48 and intragenic deletions in the wild type allele.35
ALTERNATIVE GENES IN CDH1 NEGATIVE HDGC FAMILIES
In about 70% of HDGC and 90% of FDGC families screened worldwide, CDH1 germline mutations were not identified and remain genetically unexplained. Intragenic germline deletions involving one or more exons of cancer susceptibility genes are known to be an important cause of cancer susceptibility syndromes, but are easily missed by classical PCR based mutation detection methodologies. In HDGC, intragenic mutations of CDH1 gene have only been described as second-hit inactivation mechanisms and never as germline defects.35
Since full genome linkage analysis is only feasible in very few families, strategies to identify novel genes will rely mostly on the screening of candidate genes, such as tumour suppressor genes that are commonly inactivated in sporadic gastric cancers and/or associated with gastric cancer development. Taking into account the biology of E-cadherin, obvious candidate genes for mutations are those encoding E-cadherin binding partners within the adhesion complex, namely the catenins (α, β, γ, p120ctn). The assessment of the mutational status of these genes in the setting of CDH1 negative HDGC disclosed no germline mutations, suggesting that catenins are not major susceptibility genes in HDGC.49 Two independent studies26 27 searched for germline TP53 mutations in 31 and 35 CDH1 negative gastric cancer families; two TP53 germline mutations were found, one in each study (3.2% and 2.9%, respectively).
Recently, BRCA2 germline mutations were identified in 21% of families with both gastric and breast cancer,50 and a mutation was found in one family with clustering of gastric cancer.51
We and others have ruled out RUNX3, HPP1, caspase-10 and SMAD4 as major gastric cancer predisposition genes in familial gastric cancer.26 27
OTHER MALIGNANCIES IN HDGC
Lobular breast carcinoma was shown to be over-represented in HDGC families with CDH1 germline mutations and it has been shown that female carriers of CDH1 germline mutations have a 40% lifetime risk of developing breast cancer.52
Colorectal cancer and other malignancies have been reported at very low frequencies in HDGC families.52 Noticeably, in a CDH1 positive HDGC family, one case of signet ring cell carcinoma of the colon was identified.28
HISTOPATHOLOGICAL FEATURES OF HEREDITARY DIFFUSE GASTRIC CANCER
Current knowledge on the morphological steps underlying the development of HDGC stems from detailed studies performed in 22 stomachs that were totally mapped, encompassing prophylactic gastrectomy specimens (group A)44 45 53 54 and total gastrectomies performed in patients referred from chromoendoscopic surveillance programmes (group B).54 55 In group A, prophylactic surgeries were performed in asymptomatic carriers of CDH1 inactivating germline mutations; in group B, gastrectomies were performed after the diagnosis of signet ring-cell (diffuse) carcinoma in gastric biopsies. In every specimen, at least one focus of early invasive diffuse gastric carcinoma was identified. In group A, composed mostly of members of North American families, early invasive carcinoma was not restricted to any topographic region in the stomach: foci were identified from cardia to pre-pyloric region, without evidence of antral clustering. In group B, composed of members of New Zealand Maori families, a predilection was observed for the occurrence of early invasive carcinomas for the distal stomach and the body–antral transitional zone.54 55 Reasons for the different anatomical localisation of the carcinomatous foci in the aforementioned studies remain to be clarified. To the best of our knowledge there are only two publications reporting prophylactic gastrectomies performed in CDH1 germline mutation carriers in which cancer was not identified.56 57 However, these two studies do not provide detailed data on the protocol used for the study of the surgical specimens. In our experience, unless total sampling of the whole stomachs is performed, the diagnosis of early invasive cancers can not be excluded. Actually, one of us (FC) had the opportunity to see in consultation several prophylactic gastrectomies, originally reported as negative for cancer, in which the detailed microscopic study of the whole length of gastric mucosa (after complete embedding of the whole stomach) revealed the presence of foci of early invasive signet ring-cell carcinomas in all cases (data not published).
The neoplastic cells in the early invasive cancers generally display the features of signet ring cells. In some cases a layered structure of the carcinomas is observed, the cells being small and undifferentiated at deep levels and displaying the signet ring cell phenotype at the surface. The relevance of microenvironmental factors within gastric mucosa for this polarity of morphology remains to be elucidated.
E-cadherin immunoexpression was shown to be reduced or absent in early invasive gastric carcinomas, contrasting with the normal membranous E-cadherin expression in adjacent non-neoplastic mucosa, in keeping with a clonal origin of the cancer foci.44 45
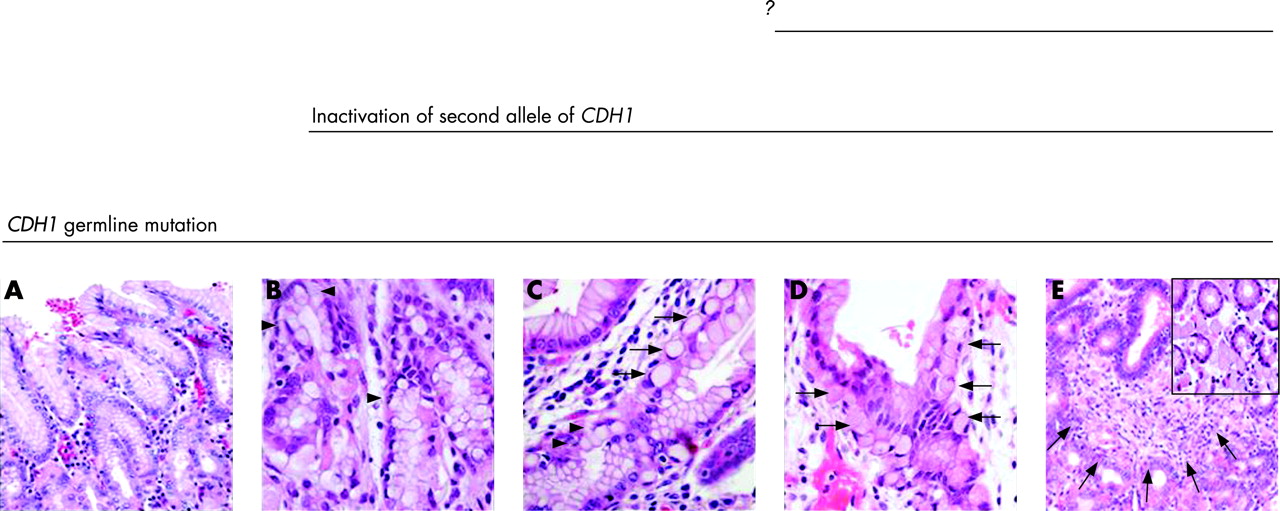
As precursors of the invasive cancers, two distinct types of lesions were identified in prophylactic gastrectomies: (i) in situ signet ring cell carcinoma, corresponding to the presence of signet ring cells within basal membrane (fig 1B,C), generally with hyperchromatic and depolarised nuclei; and (ii) pagetoid spread of signet ring cells below the preserved epithelium of glands/foveolae (fig 1C,D). In situ carcinomas are identified at the proximity of invasive carcinomas as well as in areas distant from invasive cancer. Discrepancies between the low numbers of in situ carcinomas in comparison to the number of invasive cancers suggests that invasion of the lamina propria by signet ring cells may occur without a morphologically detectable in situ carcinoma.
It is accepted that the gastric mucosa in CDH1 germline mutation carriers is normal until the second CDH1 allele is inactivated. It is postulated that this down-regulation occurs in multiple cells in the gastric mucosa, accounting for the multifocal tumour lesions. It remains to be elucidated the role played by environmental factors (diet, carcinogens), ulceration and gastritis as triggers of this down-regulation event. The genetic changes occurring after the inactivation of CDH1 remain to be elucidated.
MODEL OF DEVELOPMENT OF HEREDITARY DIFFUSE GASTRIC CANCER
On the basis of the findings in prophylactic gastrectomies, a model for the development of diffuse gastric cancer in E-cadherin mutation carriers was proposed,45 as depicted in fig 1, and encompassing the following lesions: in situ signet ring cell carcinoma, pagetoid spread of signet ring cells below the preserved epithelium of glands/foveolae, and invasive carcinoma.
Background changes in the gastric mucosa of prophylactic gastrectomy specimens encompass mild chronic gastritis, sometimes displaying the features of lymphocytic gastritis. Occasionally, an inflammatory granulomatous reaction is observed at the periphery of some collapsing glands. Foveolar hyperplasia and tufting of surface epithelium, focally with globoid change (fig 1A) is also a frequent finding and, in some areas, vacuolisation of surface epithelium is very striking.7 Additionally, erosions and cysts are common findings in non-neoplastic mucosa. In most prophylactic gastrectomies reported so far, intestinal metaplasia and Helicobacter pylori infection are absent (all from families from North America). The exception is a prophylactic gastrectomy from New Zealand in which H pylori infection was identified.54
THE ROLE OF MORPHOLOGY AS A SCREENING METHOD FOR HDGC
The identification of hereditary/familial gastric cancer is based on clinical, pathological and genetic criteria. Pathology plays a role both in the classification of familial/hereditary gastric cancer syndromes and in the identification of new cases of HDGC. The latter role has been demonstrated by Oliveira et al,58 who reported the first Portuguese family with HDGC that was identified in the study of an apparently sporadic case of early-onset diffuse gastric cancer. In this case, the gastric mucosa adjacent to widely invasive diffuse carcinoma displayed foci of in situ carcinoma and pagetoid spread of signet ring cells, similar to those previously described in HDGC.45 These findings led to additional clinical and genetic studies. A family history was confirmed and genetic testing performed, disclosing a germline CDH1 mutation in the family.58 Subsequently, genetic testing was offered to several members of this family; one member was identified as an asymptomatic carrier of CDH1 germline mutation. After genetic counselling, this individual was submitted to prophylactic gastrectomy; 14 foci of early invasive gastric cancer were identified in the surgical specimen. This case highlights the role of pathology in the identification of HDGC.
CLINICAL MANAGEMENT
In the setting of HDGC, Pharoah et al52 estimated that the cumulative risk of clinically detected gastric cancer is 67% for men and 83% for women, at the age of 80. Foci of early diffuse gastric cancer were identified in 100% of prophylactic gastrectomies reported to date, in which a detailed research protocol was used for the study of a full length of gastric mucosa. These two observations show that although CDH1 mutation carriers may develop early diffuse gastric cancer at relatively young ages, not all mutation carriers will have clinically expressed disease during their lives. At the present time, it is not possible to anticipate for how long some of the early invasive cancers will remain indolent, without clinical expression.
Efforts have been made to develop methods for early detection of diffuse gastric cancer in CDH1 germline mutation carriers in HDGC families. Chromoendoscopy with congo red/methylene blue has been found to be an improved surveillance technique in comparison to white light gastroscopy for the intensive endoscopic surveillance of CDH1 germline mutation carriers.54 59 One study claims that [18F]fluoro-2-deoxy-d-glucose positron emission tomography may facilitate early detection of HDGC,60 suggesting that further investigation of the role of this technique as a screening modality in HDGC should be performed.
Despite the advances in screening procedures for early (curable) gastric cancer, large scale studies need to be performed to confirm the usefulness of the aforementioned methods in clinical practice. Importantly, it should be taken into consideration that surveillance using endoscopy (with chromoendoscopy in some cases) and multiple mucosal biopsies have failed to identify intramucosal carcinoma in patients subjected to prophylactic gastrectomy.44 53 These findings suggest that prophylactic (total) gastrectomy should be considered as a valid approach for management of asymptomatic carriers of CDH1 germline mutations in well characterised HDGC families.28 42
In women, along with the management of gastric cancer risk, mutation carriers should be referred to a high-risk breast cancer screening programme for yearly mammographic or, preferably, MRI examinations.49
PRACTICAL APPROACH TO INDIVIDUALS AT RISK OF DEVELOPING FAMILIAL DIFFUSE GASTRIC CANCER
The clinical implications of diffuse gastric cancer associated with CDH1 germline mutations and guidelines for clinical management of familial gastric cancer have been recently reviewed by Fitzgerald and Caldas.42 61 For everyday practice, we propose a sequential approach for the diagnosis and management of individuals at risk, as depicted in fig 2.
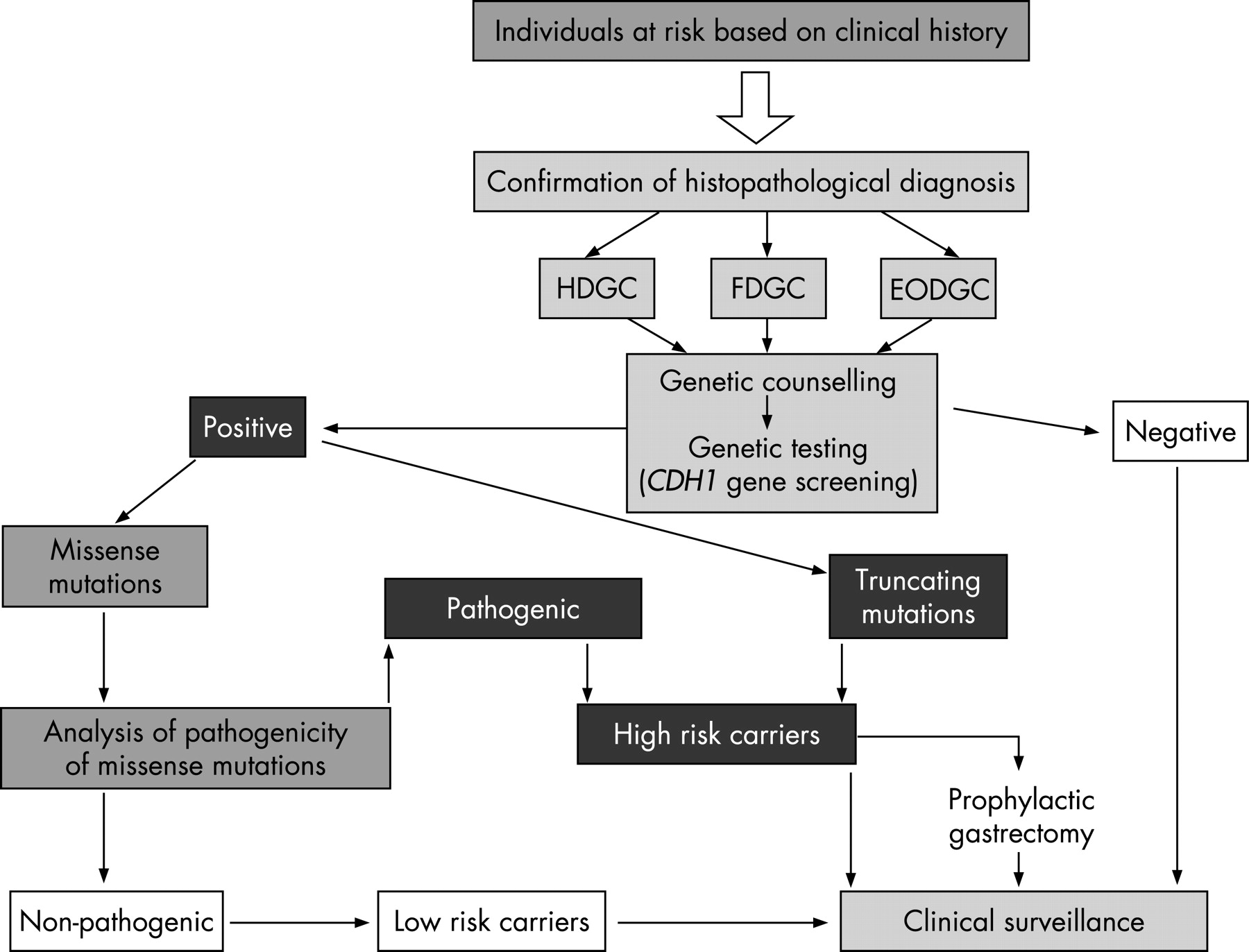
{kind=link}
{kind=link}
In the setting of HDGC caused by CDH1 germline mutations, specific recommendations were proposed by the New Zealand HDGC group regarding age dependent guidelines for genetic testing, surveillance gastroscopy and prophylactic gastrectomy.55
REFERENCES
Footnotes
Fátima Carneiro, Carla Oliveira and Raquel Seruca are members of the International Gastric Cancer Linkage Consortium (IGCLC).
Funding: The work reported here from the IPATIMUP team was partly funded by the Sixth Framework Programme from EU-FP6 (LSHC-CT-2005-018754) and the Portuguese Science Foundation (POCTI/SAU-OBS/58111/2004).
Competing interests: None declared.