Article Text

Abstract
OBJECTIVE To analyse the distributions of and generate growth charts for stature and occipitofrontal circumference (OFC) in neurofibromatosis 1 (NF1) patients.
DESIGN Cross sectional database survey.
SETTING The National Neurofibromatosis Foundation International Database (NFDB) includes clinical information on NF1 patients from 14 participating centres in North America.
SUBJECTS A total of 569 white, North American, NF1 patients, 55% female and 45% male.
MAIN OUTCOME MEASURES Stature and OFC measurements of NF1 patients were compared to age and sex matched population norms using z score standardisation and centile curves.
RESULTS The distributions of stature and OFC are shifted and unimodal among NF1 patients; 13% of patients have short stature (⩾2 standard deviations below the population mean) and 24% have macrocephaly (OFC ⩾2 standard deviations above the population mean).
CONCLUSIONS Alterations of stature and OFC are not limited to NF1 patients with frank short stature or macrocephaly.
- neurofibromatosis 1
- stature
- occipitofrontal circumference
- macrocephaly
Statistics from Altmetric.com
Neurofibromatosis 1 (NF1) is an autosomal dominant disorder affecting about 1 in 3000 people.1-3 Its most frequent features are café au lait macules, iris Lisch nodules, and discrete and plexiform neurofibromas. Short stature (⩾2 SD below the population mean) and macrocephaly (⩾2 SD above the population mean) are more common in people affected with NF1 than in the general population.4-7
NF1 features such as scoliosis and early or delayed puberty occasionally influence stature. However, short stature associated with NF1 usually affects the whole skeleton proportionately, and no specific cause is apparent in most cases.5 8 Disease features such as hydrocephalus and plexiform neurofibromas occasionally affect measurements of occipitofrontal circumference (OFC). However, increased OFC among NF1 patients usually has no obvious cause and appears to result from overgrowth of the brain.5 8
It has been suggested that short stature and macrocephaly are “all or none” phenomena that affect only a subset of NF1 patients.5 According to this hypothesis, NF1 patients would be expected to fall into two distinct groups: (1) those whose stature is in the same normal distribution as unaffected people of the same age, and (2) those whose stature is decreased. NF1 patients would also be expected to fall into two distinct groups with respect to macrocephaly: (1) those whose OFC is in the same normal distribution as unaffected people of the same age, and (2) those whose OFC is increased. We examined the distributions of these measurements to determine whether changes in growth affect all or only a subset of patients with NF1. We also generated centile curves for stature and OFC by age and gender.
Subjects and methods
SUBJECTS
All patients included in this study meet the NIH Diagnostic Criteria for NF1.9 10 Measurements of patient stature and OFC were obtained from the National Neurofibromatosis Foundation International Database (NFDB).11 At the time of this analysis, the NFDB included extensive demographic and cross sectional clinical and anthropometric data on 569 North American, white, NF1 patients examined during 1980-1998 at 14 participating centres in North America. Information was collected and recorded on each patient using a standard procedure. Patient stature was measured without shoes using a stadiometer. OFC was measured at the largest diameter over the occiput and forehead using an inextensible tape line measure. The data were subjected to automated range checking and routinely screened for quality and consistency by the database administrator. Only measurements from each patient's first visit to a participating clinic were included in the analysis. Patients who were known to have one or more of the following features on any clinical visit were excluded from analyses of stature: pseudarthrosis (n=22, 3%), early (under 10 years) (n=13, 2%) or delayed (over 15 years) (n=51, 1%) puberty, optic glioma (n=66, 9%), scoliosis (n=98, 14%), or vertebral dysplasia (n=19, 3%). The final sample for analyses of stature consisted of 183 males and 202 females. Patients with one or more of the following features were excluded from analyses of OFC: plexiform neurofibroma of the head (n=46, 6%), early or delayed puberty, optic glioma, or hydrocephalus (n=23, 3%). The ultimate sample for analyses of OFC consisted of 216 males and 220 females.
REFERENCE POPULATIONS
Standard population norms for stature by age were obtained from the National Center for Health Statistics (NCHS) studies during 1963-1974.12 The NCHS standards are based on a sample consisting of 83% percent white or Hispanic subjects and 17% percent black subjects living in the United States. Standard population norms for OFC by age were obtained from the Fels Institute study conducted during 1929-1975.12 The Fels Institute sample is slightly less heterogeneous than the NCHS sample.
DISTRIBUTION ANALYSIS
Stature and OFC measurements were standardised using z scores to control for both age and gender:

Patients with stature and OFC measurements corresponding to a z score with an absolute value greater than 7 were excluded to minimise data entry errors. Four (1%) stature and two (0.5%) OFC measurements corresponded to z scores below −7. One (0.3%) stature and two (0.5%) OFC measurements corresponded to z scores above 7. Single data entry, as used in this study, has an error rate around 2%.13-15 After these exclusions, we expect that about 1% of the remaining measurements contain errors.
We tested the standardised data by analysis of variance to determine if significant differences exist among the measurements made by the major contributing centres.
Distributions of z scores for stature and OFC were plotted in histograms using SAS.16 Each histogram is based on the z scores compiled from males and females of all ages. In addition, the deviation from unimodality of each distribution was quantified by computing its dip statistic.17 Dip approaches zero for unimodal distributions. The significance of a given dip value is determined by comparing it to the distribution of values from a known unimodal distribution.
GROWTH CURVES
Centiles were generated directly from the data for NF1 patients of various ages and compared to the corresponding centiles from reference populations. NF1 patients were divided into sex and age groups matching those of the curves available for population norms. A typical series of age groups had medians of 2, 2.5, 3 . . .18 years. Age group limits were determined by splitting the difference between a given median and the next lowest and highest medians. Patients with ages equidistant from two medians were assigned to the older age group. For example, the 2.5 year old group included patients aged 2.250 to 2.749 years old. The 5th, 25th, 50th, 75th, and 95th centiles for stature and OFC were determined for each sex in each age group of NF1 patients and plotted alongside the centiles from the corresponding population standards. The data were plotted and smoothed using SAS.16 Smoothing was done by producing a cubic spline that minimises a linear combination of the sum of squares of the residuals of fit and the integral of the square of the second derivative.16 18 Smoothed curves were inspected to ensure that the final results reasonably represent the data. Splining was used and described in detail by Hamill et al 12 to generate standard curves for the NCHS.
Results
A total of 183 males and 202 females were included in analyses of stature and 216 males and 220 females were included in analyses of OFC. Analysis of variance for heterogeneity among the 14 North American contributing centres showed no centre bias for age and sex standardised stature (p=0.72) or OFC (p=0.10).
Figs 1 and 2 show the distributions of standardised measurements of stature and OFC among NF1 patients and population norms. Mean standardised stature among NF1 patients is lower than the mean in the reference population. Thirteen percent of the NF1 patients lie 2 SD or more below the reference population mean, compared to 2% of norms. Mean standardised OFC among NF1 patients is greater than the mean in the reference population. Twenty four percent of NF1 patients lie 2 SD or more above the reference population mean.

Distribution of sex and age standardised stature. NF1 patient measurements are from the National NF Foundation Database. Unaffected norms are from the National Center for Health Statistics and the Fels Institute.
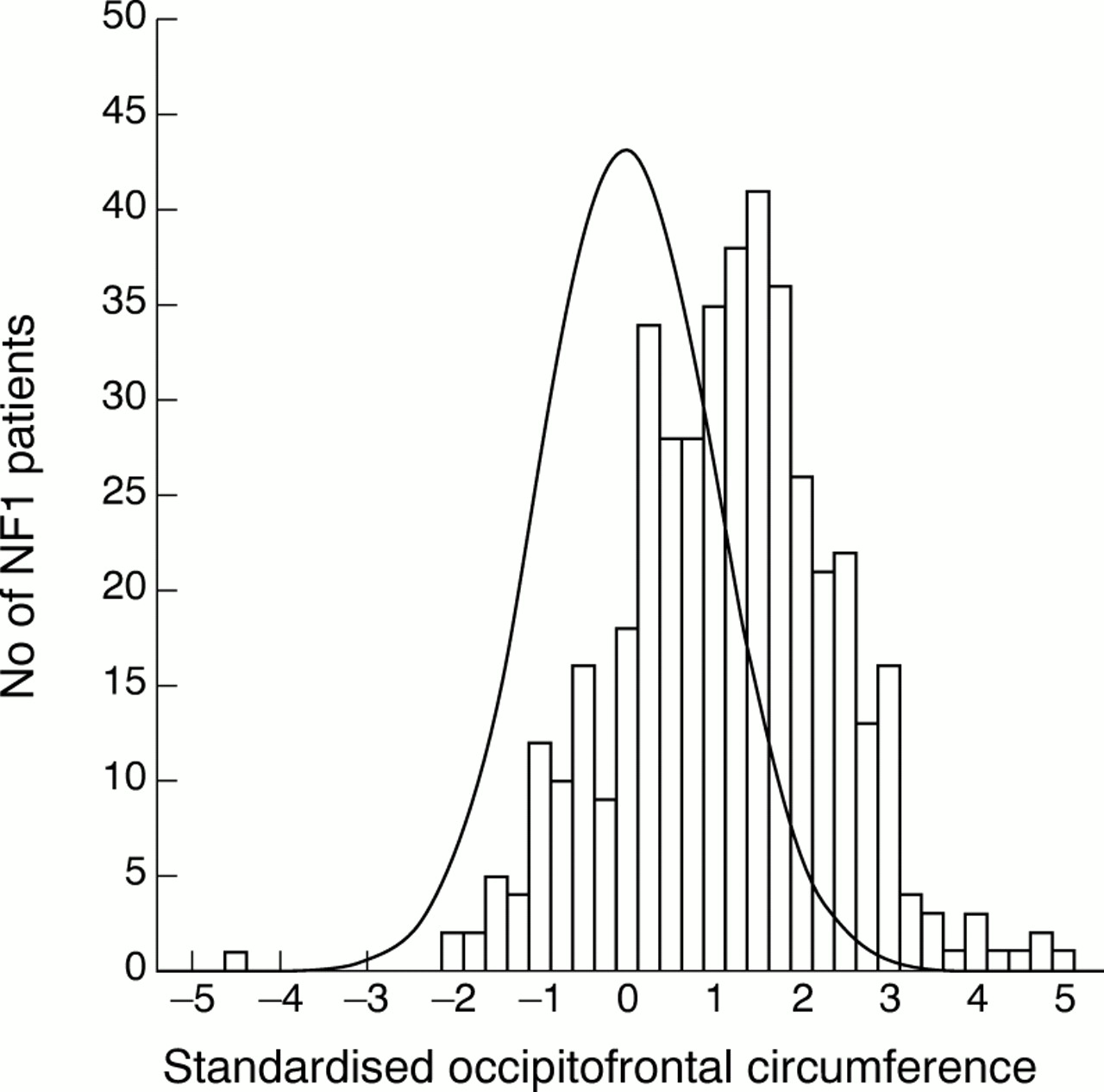
Distribution of sex and age standardised occipitofrontal circumference. NF1 patient measurements are from the National NF Foundation Database. Unaffected norms are from the National Center for Health Statistics and the Fels Institute.
The histograms for stature and OFC appear unimodal (figs 1 and 2); their dip statistics, which measure departures from unimodality, are 0.014 and 0.012, respectively. These correspond to the 5th centiles of departures from known unimodal distributions. In other words, the deviations are either within the normal range for known unimodal distributions or lower. The standardised stature distribution has a skewness of 0.32 and a kurtosis of 0.19; most of the cases are clustered to the left of the mean and the distribution peaks more abruptly than a normal distribution. The standardised OFC distribution has a skewness of −0.16 and a kurtosis of 0.87; most of the cases are to the right of the mean and the distribution peaks more abruptly than normal.
Stature and OFC centiles by age are shown in figs 3 and 4. Median stature is as much as 7 cm lower and OFC 2 cm greater in our NF1 patients than in the standard paediatric growth charts, depending on age and gender.
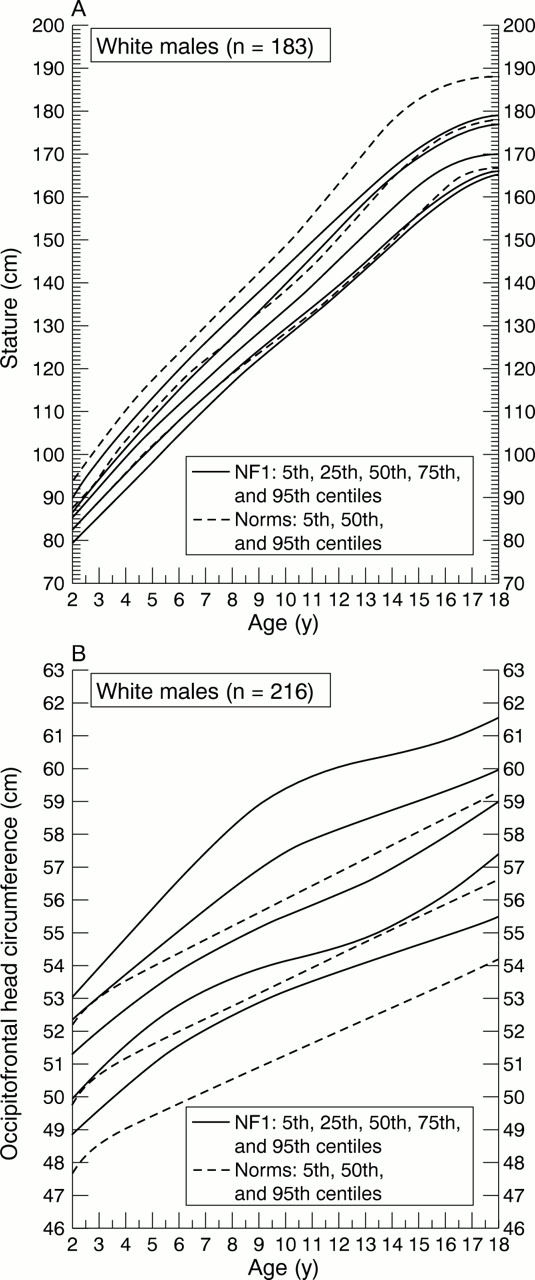
(A) Stature centiles in males 2-18 years. NF1 patient measurements are from the National NF Foundation Database and are denoted by solid lines. Unaffected norms are from the National Center for Health Statistics and the Fels Institute and are denoted by dashed lines. (B) Occipitofrontal circumference centiles in males 2-18 years. NF1 patient measurements are from the National NF Foundation Database and are denoted by solid lines. Unaffected norms are from the National Center for Health Statistics and the Fels Institute and are denoted by dashed lines.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
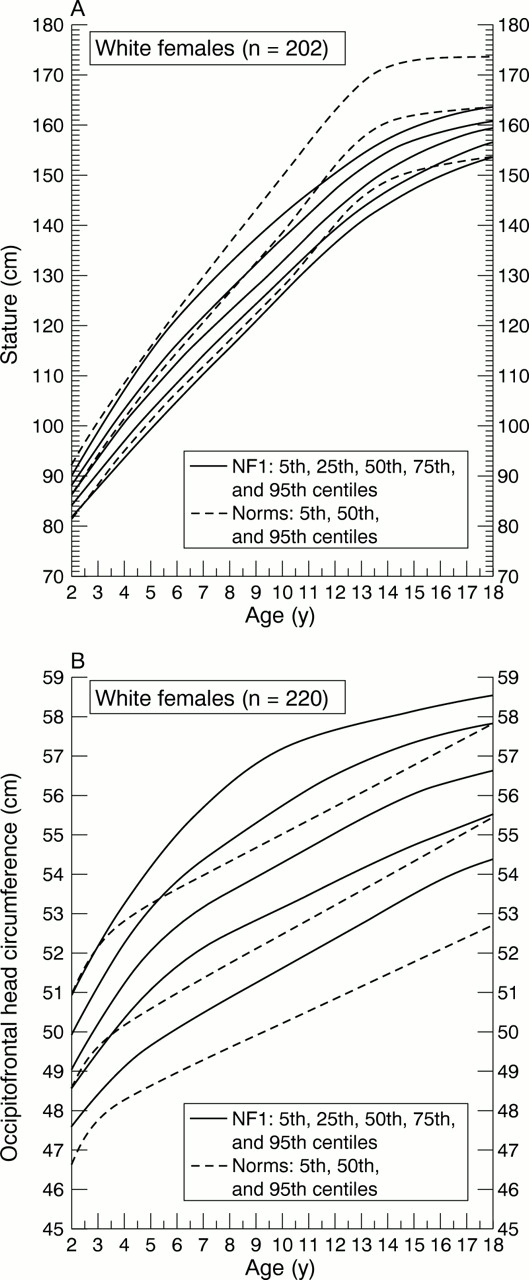
(A) Stature centiles in females 2-18 years. NF1 patient measurements are from the National NF Foundation Database and are denoted by solid lines. Unaffected norms are from the National Center for Health Statistics and the Fels Institute and are denoted by dashed lines. (B) Occipitofrontal circumference centiles in females 2-18 years. NF1 patient measurements are from the National NF Foundation Database and are denoted by solid lines. Unaffected norms are from the National Center for Health Statistics and the Fels Institute and are denoted by dashed lines.
Discussion
The NCHS and Fels standards were used for comparison to stature and OFC of NF1 patients because these studies cover a wide range of ages and are commonly used clinically to diagnose short stature and macrocephaly. These normal population studies were longitudinal and therefore more accurately represent growth than the cross sectional studies we used. More recent NCHS standards for boys and girls are available for stature, but not for occipitofrontal circumference (http://www.cdc.gov/growthcharts). These new stature standards for boys and girls are remarkably similar to the ones we used.12 19
Standardisation for age and sex by z scores is a transformation that allows pooling of measurements across groups that differ in age and sex. This transformation can be applied to measurements for which standard population distributions are approximately normal. The distributions of stature and OFC satisfy this criterion.12Thus, a subject's z score closely corresponds to his or her centile rank.
We were concerned that differences between centres would increase the variability of our sample and diminish our ability to analyse the standardised distributions. However, analysis of variance detected no differences for stature or OFC among the contributing centres.
The shifts in the standardised distributions of stature and OFC (figs 1and 2) confirm that, on average, our NF1 patients are shorter and have bigger heads than standard populations. The shifts are very similar to those in a recent longitudinal study by Carmi et al.20 The population norms were not taken during the same years as our sample, and some were taken 20 or more years earlier. Secular trends suggest that stature and OFC may have increased in the normal population over this time.16 21-23 If year specific standards were used in our study and the one by Carmiet al,20 the shift in stature may be slightly larger than indicated here and the shift in OFC may be slightly smaller. Ascertainment bias may also affect the distribution shifts. Although short stature and macrocephaly are not among the diagnostic criteria for NF1, these features may have contributed to the patients' referral to the contributing NF clinics.9Therefore, the group in this study may be shorter and have bigger heads than a population based sample of children with NF1.
The distributions of standardised stature and OFC are more abruptly peaked than a normal distribution, indicating a relative excess of cases around the mean and in the tails. This variability could result from several factors. (1) The NFDB patient measurements are cross sectional and, therefore, more variable than longitudinal data. (2) Our patient group is geographically heterogeneous. (3) A small proportion of cases may have data entry errors. (4) Ascertainment bias may increase the frequency of outliers. (5) Such distributions might represent composites of more than one normally distributed group with the same mean but different variances.24
Riccardi5 has suggested that short stature and macrocephaly in NF1 are “all or none” phenomena, that is, that two different groups of NF1 patients exist, those with short stature (or macrocephaly) and those without. Under this hypothesis, the distributions should be bimodal, with one mode more than 2 SD outside the normal mean. Our findings are not consistent with this suggestion. The distributions (figs 1 and 2) indicate that stature is reduced to some degree and OFC enlarged to some extent in all NF1 patients.
Our centile curves for stature and OFC (figs 3 and 4) are comparable to those from a recent study of Italian NF1 patients.25 Minor differences may be partly because of line smoothing techniques and geographical variation. Deviation from these NF1 standards may indicate the effect of a specific disease feature such as optic glioma or hydrocephalus. NF1 specific charts may also provide reassurance that an affected child's growth, although outside the “normal” range on standard paediatric growth charts, is actually normal for a child with NF1. Charts for body mass index and the ratio OFC/stature by age and gender in white NF1 patients are available fromhttp://www.medgen.ubc.ca/friedmanlab.
Patients with hydrocephalus and plexiform neurofibromas of the head were excluded from analyses of OFC, so enlargement of the head in the remaining patients must be the result of enlargement of the scalp, skull, or brain. In NF1, enlargement of the brain is the probable cause.5 8 Glial cell proliferation is increased in vitro by sera from NF1 patients, compared to sera from unaffected subjects.26 Optic or other CNS gliomas are another manifestation of glial cell proliferation. They were observed by MRI in 10% of people in the NFDB affected with NF1. Other studies have observed optic gliomas in 1.5% of 135 and 15% of 217 NF1 patients.27 28 Glial overgrowth is an important part of NF1 and it may be responsible for macrocephaly in NF1 patients.
Patients with puberty disturbance or bone abnormalities were excluded from analyses of stature. The cause of the stature reduction in the remaining NF1 patients is unknown, but it appears to affect the skeleton proportionately.5 Data reviewed by Howellet al 29 indicate that growth hormone replacement therapy resulted in a moderate increase in stature for NF1 patients with biochemical evidence of growth hormone deficiency. However, growth hormone deficiency was found in only three (2.5%) of 122 children with NF1 in another study.30 Short stature occurs much more frequently (13%) in the NFDB than can be attributed to such deficiency. Although growth hormone levels were not measured routinely in the NFDB patients, less than 1% are known to have ever had documented growth hormone deficiency.
The findings in this study are consistent with known molecular function of the NF1 gene/protein. The NF1 protein, neurofibromin, is involved in control of cellular growth and differentiation through the interaction of its GAP related domain with p21ras and tubulin.31 Neurofibromin is expressed in many different tissues, including the brain, and mutations in the GAP related domain produce hyperactivity of p21ras, which leads to aberrant signalling for cell proliferation.32 This may contribute to increased glial (astrocyte) cell proliferation and to enlargement of the brain in NF1 patients.32 33
The NF1 homologue inDrosophila acts as an activator of the cAMP pathway as well as a negative regulator of Ras.34 Drosophila homozygous for either of two particular NF1 mutants that lack expression of NF1 protein are 20 to 25% smaller than flies of the parental strain.35 This growth defect was rescued not only by anNF1 transgene but also by expression of activated protein kinase A, suggesting protein kinase A functions downstream of or parallel to neurofibromin. Deficiencies in this pathway may contribute to a smaller phenotype in humans as well. Activated protein kinase A is known to stimulate proliferation in some cell types and may normally contribute to body growth.36 37 Normal stimulation of the protein kinase A pathway also accelerates differentiation and inhibits proliferation of glial (oligodendrocyte) cells.38 39 Neurofibromin involvement in or between the protein kinase A and p21ras pathways may contribute to the larger heads observed in people diagnosed with NF1.40 However, our patients with the smallest stature did not also have the largest heads (results not shown).
Short stature and macrocephaly are well recognised clinical features of NF1. This study suggests that these changes in growth affect all NF1 patients and are not limited to particular subgroups. The mechanisms by which mutations of the NF1 gene produce these phenotypic effects are unknown, but understanding how they do so may provide an important clue to the pathogenesis of more serious manifestations of NF1.
Acknowledgments
This work was supported in part by the Department of the Army, USAMRMC, grant number NF960003, the National Neurofibromatosis Foundation, and the British Columbia Neurofibromatosis Foundation.
References
Footnotes
-
↵* Wylie Burke, Robin Bennett (University of Washington, Seattle), J M de Campos (Fundacion Jimenez Diaz, Madrid), J M Friedman, Patricia Birch (University of British Columbia), Bruce Korf (Boston Children's Hospital), Wilma Krause, Kim Uhas (Scottish Rite Children's Medical Center, Atlanta), Michihito Niimura, Yoshikata Inaba (Jikei University, Tokyo), Kathryn North (Children's Hospital, Sydney, Australia), June Ortenberg, Vazken Der Kaloustian (Montreal Children's Hospital), Minna Poyhonen (Oulu University Hospital, Finland), Allan Rubenstein (Mount Sinai Medical Center, New York), Priscilla Short, Kathleen Bové (Massachusetts General Hospital), Susan Stine, Linda Nicholson (Dupont Institute, Wilmington), Romano Tenconi (University of Padova, Italy), Elaine Zackai (Children's Hospital of Philadelphia), John Carey, David Viskochil (University of Utah Medical Center, Salt Lake City), Nikolay Bochkov (I M Sechenov Moscow Medical Academy, Russia), Elizabeth Schorry (Children's Hospital, Cincinnati), Sigrid Tinschert (Institut für Medizinische Genetik, Berlin), Thaddeus Kelly (University of Virginia Medical Center, Charolettesville), Jana Klein (Cedars-Sinai Medical Center, Los Angeles), Eniko Pivnick (Le Bonheur Children's Medical Center, Memphis), Alison Colley (Newcastle Western Suburbs Hospital, Australia), Marcus Schülke (Freien Universität Berlin), Mauro Signorini (Clinica Pediatrica dell'Universita, Italy), Pierre Wolkenstein (Hopital Henri-Mondor, France), Adrian Danek (Neurologische Universitaetsklinik, Muenchen, Germany).