Article Text

Abstract
Background Risk-reducing salpingo-oophorectomy (RRSO) is the most effective intervention to prevent ovarian cancer (OC). It is only available to high-risk women with >10% lifetime OC risk. This threshold has not been formally tested for cost-effectiveness.
Objective To specify the OC risk thresholds for RRSO being cost-effective for preventing OC in premenopausal women.
Methods The costs as well as effects of surgical prevention (‘RRSO’) were compared over a lifetime with ‘no RRSO’ using a decision analysis model. RRSO was undertaken in premenopausal women >40 years. The model was evaluated at lifetime OC risk levels: 2%, 4%, 5%, 6%, 8% and 10%. Costs and outcomes are discounted at 3.5%. Uncertainty in the model was assessed using both deterministic sensitivity analysis and probabilistic sensitivity analysis (PSA). Outcomes included in the analyses were OC, breast cancer (BC) and additional deaths from coronary heart disease. Total costs and effects were estimated in terms of quality-adjusted life-years (QALYs); incidence of OC and BC; as well as incremental cost-effectiveness ratio (ICER).
Data sources Published literature, Nurses Health Study, British National Formulary, Cancer Research UK, National Institute for Health and Care Excellence guidelines and National Health Service reference costs. The time horizon is lifetime and perspective: payer.
Results Premenopausal RRSO is cost-effective at 4% OC risk (life expectancy gained=42.7 days, ICER=£19 536/QALY) with benefits largely driven by reduction in BC risk. RRSO remains cost-effective at >8.2% OC risk without hormone replacement therapy (ICER=£29 071/QALY, life expectancy gained=21.8 days) or 6%if BC risk reduction=0 (ICER=£27 212/QALY, life expectancy gained=35.3 days). Sensitivity analysis indicated results are not impacted much by costs of surgical prevention or treatment of OC/ BC or cardiovascular disease. However, results were sensitive to RRSO utility scores. Additionally, 37%, 61%, 74%, 84%, 96% and 99.5% simulations on PSA are cost-effective for RRSO at the 2%, 4%, 5%, 6%, 8% and 10% levels of OC risk, respectively.
Conclusions Premenopausal RRSO appears to be extremely cost-effective at ≥4% lifetime OC risk, with ≥42.7 days gain in life expectancy if compliance with hormone replacement therapy is high. Current guidelines should be re-evaluated to reduce the RRSO OC risk threshold to benefit a number of at-risk women who presently cannot access risk-reducing surgery.
- Ovarian cancer
- risk reducing salpingo-oophorectomy
- risk threshold
- surgical prevention
- cost-effectiveness
Statistics from Altmetric.com
- Ovarian cancer
- risk reducing salpingo-oophorectomy
- risk threshold
- surgical prevention
- cost-effectiveness
Introduction
Ovarian cancer (OC) remains the top most cause of gynaecological cancer mortality,1 with 152 000 deaths occurring worldwide annually.2 The best method for preventing OC in women at high risk of this disease is premenopausal risk-reducing salpingo-oophorectomy (RRSO). This is usually undertaken in women aged >35 years, who have completed their family.3 The importance of surgical prevention is further magnified as the effectiveness of OC screening is still not established.4–6 RRSO is associated with an OC HR of 0.21 (CI 0.12 to 0.39)3 for BRCA1/2 mutation carriers and 0.06 (CI 0.02 to 0.17) for lower-risk populations.7 RRSO is not currently offered to women at <10% lifetime risk of OC, but only available to those at ‘high risk’, such as BRCA1/2 carriers, for whom this strategy is found to be cost-effective.8
The cost-effectiveness of ‘premenopausal RRSO’ as a prevention strategy at lower than BRCA1/BRCA2 risk levels remains to be properly assessed. Although we recently addressed this issue in postmenopausal women,9 the precise ‘risk threshold’ at which ‘premenopausal RRSO’ would be cost-effective to prevent OC is yet to be specified. First-degree relatives (FDRs) of women with epithelial OC have a threefold higher risk of developing OC.10 Additionally of late, newer intermediate/moderate risk genes like RAD51C,11 RAD51D12 and BRIP113 have been identified. Validation data confirming their penetrance estimates have recently been published,14 ,15 and are likely to lead to clinical testing in the near future. A significant proportion of these cancers occur in the premenopausal age group. Furthermore, genome-wide association studies have led to the discovery of 17 common genetic variants modifying OC risk.16 ,17 Women carrying multiple risk variants have a higher OC risk compared with women with a lower polygenic load. Recently, we reported an OC risk prediction algorithm,18 which incorporates BRCA1/2, as well as common genetic variants and other familial effects, thus permitting more accurate risk prediction in BRCA1/2-negative women.
We hypothesise that premenopausal RRSO will turn out to be cost-effective to prevent OC at lower risk levels that are associated with mutations in intermediate/moderate penetrance genes and/or combination of familial/common variant genetic risk factors. Recognised, proven published data are used to illustrate a decision analysis model19 comparing ‘RRSO’ and ‘no RRSO’ in premenopausal women across a range of OC risks (2–10%) to identify the lifetime risk level(s) for RRSO to be undertaken for OC prevention.
Methods
A decision analysis model was built in order to evaluate lifetime costs as well as effects with undertaking ‘RRSO’ in 40-year-old premenopausal women by comparing it with ‘no RRSO’ at varying levels of OC risk ranging from 2% to 10% within the UK National Health Service (NHS) context. This is consistent with advice from the National Institute for Health and Care Excellence (NICE), which recommend using a cost-effectiveness analysis as the preferred method of economic evaluation to compare the relative health outcomes and costs of interventions.20 The model (figure 1) was programmed in Microsoft Excel and run at varying (2%, 4%, 5%, 6%, 8% and 10%) lifetime risk levels for OC. The baseline breast cancer (BC) risk (12.9%) was obtained from population-based data.21 Screening for OC is not included in the model as a mortality benefit is yet to be demonstrated and it is not available on the NHS.9 Two large studies7 ,22 have reported an increased mortality associated with premenopausal bilateral oophorectomy. This was seen primarily in those who underwent oophorectomy at ages <4522–507 years but did not get hormone replacement therapy (HRT). Following RRSO, it is recommended that all premenopausal women take HRT till the median age of menopause, 51 years. We assumed that 80% (CI 76% to 83%) of women were compliant23 and costed/modelled this accordingly.
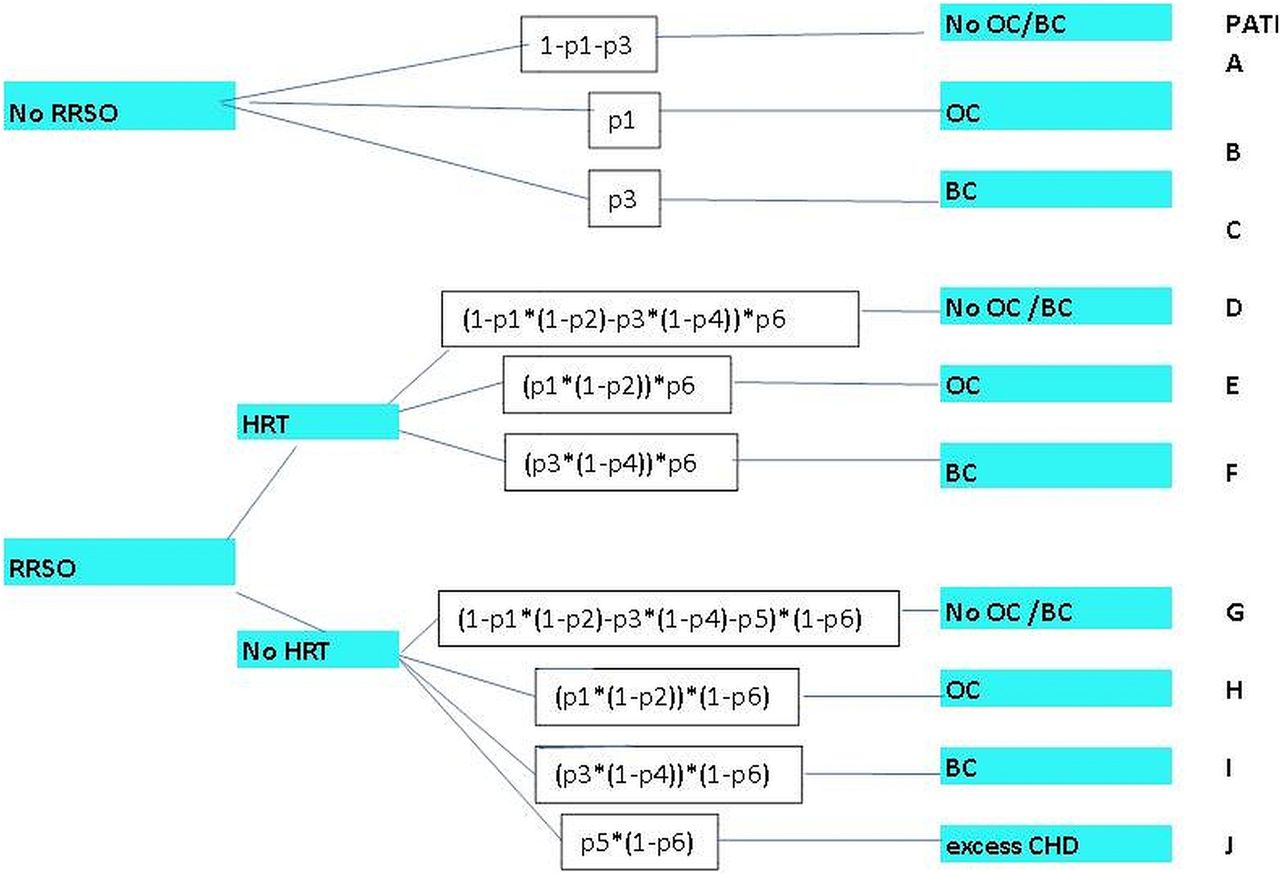
Decision model structure. The upper part of the model structure reflects outcomes of not undergoing risk-reducing salpingo-oophorectomy (RRSO) and the lower part of the model depicts premenopausal RRSO. This model is run at each of the different thresholds for ovarian cancer (OC) risk (2%, 4%, 5%, 6%, 8%, 10%). Each decision point in the model is called a ‘node’, and each path extending from a node is called a decision ‘branch’. Each branch represents a mutually exclusive course or outcome. Each decision is given a probability (probabilities ‘p1 to p6’ used in the model are explained in table 1) highlighted in a white box along the decision branch. Values for each outcome are calculated. Cancer incidence was estimated by summing the probabilities of pathways ending in ovarian or breast cancer. Final outcomes (blue boxes on the right of the figure) of each path include development of breast cancer (BC), OC, no BC/OC and excess deaths from coronary heart disease (CHD). HRT, hormone replacement therapy
Figure 1 reflects outcomes of the decision model dependent on whether RRSO is undertaken or not. The upper part depicts outcomes without RRSO. Each point where a decision is made is termed a ‘node’. The line stretching out from the ‘node’ is termed a decision ‘branch’, which in turn denotes a mutually exclusive course/outcome. All decisions are assigned a probability and all outcomes were computed accordingly. Costs for identifying/calculating OC risk were not included and were assumed to have been identified through existing algorithms. Outcomes included OC, BC, as well as additional deaths due to coronary heart disease (CHD). As recommended by NICE, the discounted value used for all outcomes as well as costs was 3.5%.20
Probabilities
Probabilities assigned to different pathways in the model are provided in table 1. It was assumed that short-term HRT following RRSO did not affect BC risk.24 The reduction in OC and BC risk from RRSO, and the additional CHD deaths were obtained from the Nurses Health Study.7 They described an absolute increase in CHD mortality of 3.03% with the number needed to harm being 1:33. The probabilities of all paths/branches leading to OC or BC were summed up to estimate cancer incidence. The chance of both BC and OC occurring at the same time is rare and assumed to be close to zero.
Probabilities of pathways in the model
Costs
All costs (table 2) were derived from a healthcare system (UK NHS)/payer's perspective and reported at 2012 prices.25 The Hospital and Community Health Service Index was used to convert these costs as needed.26 As advised by NICE, future healthcare costs that are not related to OC/BC were not included.20
Costs used in the model (2012 prices)
Supplemental material
Life-years
The time horizon in the study covers lifetime risks and long-term consequences. Office of National Statistics life tables were used to obtain female life expectancy estimates for women who do not get OC or BC.27 The median ages of onset of OC/BC were 68/60 years, respectively (from Cancer Research UK).28 BC and OC outcomes were modelled using 10-year survival estimates. The 1-year, 5-year and 10-year survival rates for women who develop OC are 72.4% (CI 72.4% to 72.5%), 46.2% (CI 45.9% to 46.4%) and 34.5% (CI 33.8% to 35.3%), respectively.29 For BC: 1-year survival=96% (CI 96% to 96%); 5-year survival rate=86.6% (CI 86.6% to 86.6%); 10-year survival=78.4% (CI 78.3% to 78.4%).30 The probability of dying after 10-year survival was presumed to be similar to the rest of the population.
Quality-adjusted life-years
Quality-adjusted life-years (QALYs) is recommended by NICE as the most appropriate determinant of health benefit, which reflects mortality and health associated quality-of-life effects.20 QALY expresses change in life expectancy , which incorporates a potential declining quality of life. This necessitates information on utility weights (also called utility scores). ‘Utility weights’ indicate an individual's choice using a 0–1 scale for particular health states, where ‘1’ implies ‘perfect health’ while ‘0’ implies death. Utility weight reflects the quality-of-life-based adjustment made for different health states included in the model. QALY=(survival in life-years)× (utility weight)31 for RRSO is reported to have a utility score estimate of 0.95 (SD=0.1, Grann32) and for OC treatment health states were obtained from Havrilesky.33 Visual scales that compare health state preferences are intrinsically biased and usually less precise34 Hence, time trade-off scores were used by us. Seventy percent women present with advanced stage newly diagnosed OC,35 ,36 with a lower utility score=0.55 (SD=0.29). The utility score for those with early-stage OC is 0.81 (SD=0.26) and much greater than the utility score of 0.16 (SD=0.25) for women with OC who are at their end stage of life (last year of life).. The annual recurrence rate for women with early-stage OC who survive initial chemotherapy is 10.5%,37 while the recurrence rate for advanced stage disease is 20.6%.35 The mean utility score for women in whom OC recurs is 0.5 (range 0.4–0.61), whereas the score for those in remission is=0.83 (SD=0.25).31 ,33
One in ten (10%) cases of BC are non-invasive/DCIS and 90% of BC are invasive. Of invasive BC, 95% is early and locally advanced, of which 41% is stage 1, 45% is stage 2 and 9% is stage 3.21 ,38–40 While 5% of invasive BC is advanced (stage 4).21 ,38 ,39 Utility weights for BC were obtained from NICE guidelines.41 ,42 This was assumed to be 0.65 for advanced BC=0.71 for early/locally advanced BC=0.81 for remission and 0.45 for recurrence. After surviving initial chemotherapy, 35% of early/locally advanced39 and 66% of advanced BC cases will recur/progress.43
Analysis
The path probabilities were multiplied to compute the chance for existing in each of the model branches. The values for each branch in the model were weighted by the probability of being in each branch to calculate overall costs and effects from the model described in life-years and QALYs. The incremental cost-effectiveness ratio (ICER) is described as the overall difference in cost divided by the difference in effect. ICER=(cost of ‘RRSO’ – cost of ‘no-RRSO’)/(effect of ‘RRSO’ – effect of ‘No-RRSO’). The ICER obtained was then compared with the standard cost-effectiveness thresholds of £20 000–£30 000/QALYs recommended by NICE.31 ,44 This was used to determine whether undertaking ‘premenopausal RRSO’ is cost-effective in contrast to ‘no RRSO’ at the different OC risk thresholds. An extensive sensitivity analysis was undertaken to explore any uncertainty in the results as well as model robustness. Each individual parameter in the model was varied in a deterministic (one-way) sensitivity analysis and the model rerun to evaluate influence on results. Model probabilities/utility weights were altered and analysed at extremes of their 95% CI or range, wherever accessible, or by ±10%, while all costs used in the model were altered by ±30%.31 However, model probabilities or parameters are likely to fluctuate simultaneously in parallel and not individually. Hence, additionally as per NICE recommendations, we also performed probabilistic sensitivity analysis (PSA),20 ,45 where uncertainty in the model is explored by varying all variables simultaneously across their distributions. Appropriate distributions were fitted in the PSA such as ‘beta’ for probabilities, ‘gamma’ for costs as well as ‘log normal’ for utilities as suggested in the literature.46 Results of 1000 simulations were plotted by a cost-effectiveness acceptability curve. It depicted the proportion of simulations showing RRSO was cost-effective at varying ‘OC risk’ and £20 000 as well as £30 000 ‘willingness-to-pay’ thresholds.
Results
Undiscounted and discounted survival time in terms of life-years/QALYs as well as overall costs and cancer incidence obtained at different OC risk thresholds (2–10%) are given in table 3. The overall cost difference as well as gain in life-years/QALYs is smaller following discounting. This is because costs/outcomes that happen in the future are adjusted by discounting and cost savings that are generated through preventing future OC cases are therefore valued less. Premenopausal RRSO was highly cost-effective at 4% OC risk with 42.7 days gain in life expectancy at an ICER=£19 536/QALY. At the baseline 2% OC risk, premenopausal RRSO is not cost-effective for £30 000/QALY threshold (ICER=£46 480/QALY, 19.9 days gain in life expectancy). These benefits are to a large extent driven by the significant advantage obtained from reduction in BC risk and HRT compliance rate. Modelling shows that cost-effectiveness increases with corresponding rises in thresholds for OC risk.
Model outcomes for costs, survival (life-years) and quality-adjusted life-years (QALYs), undiscounted and discounted (including benefit of reduction in breast cancer risk from premenopausal risk-reducing salpingo-oophorectomy (RRSO))
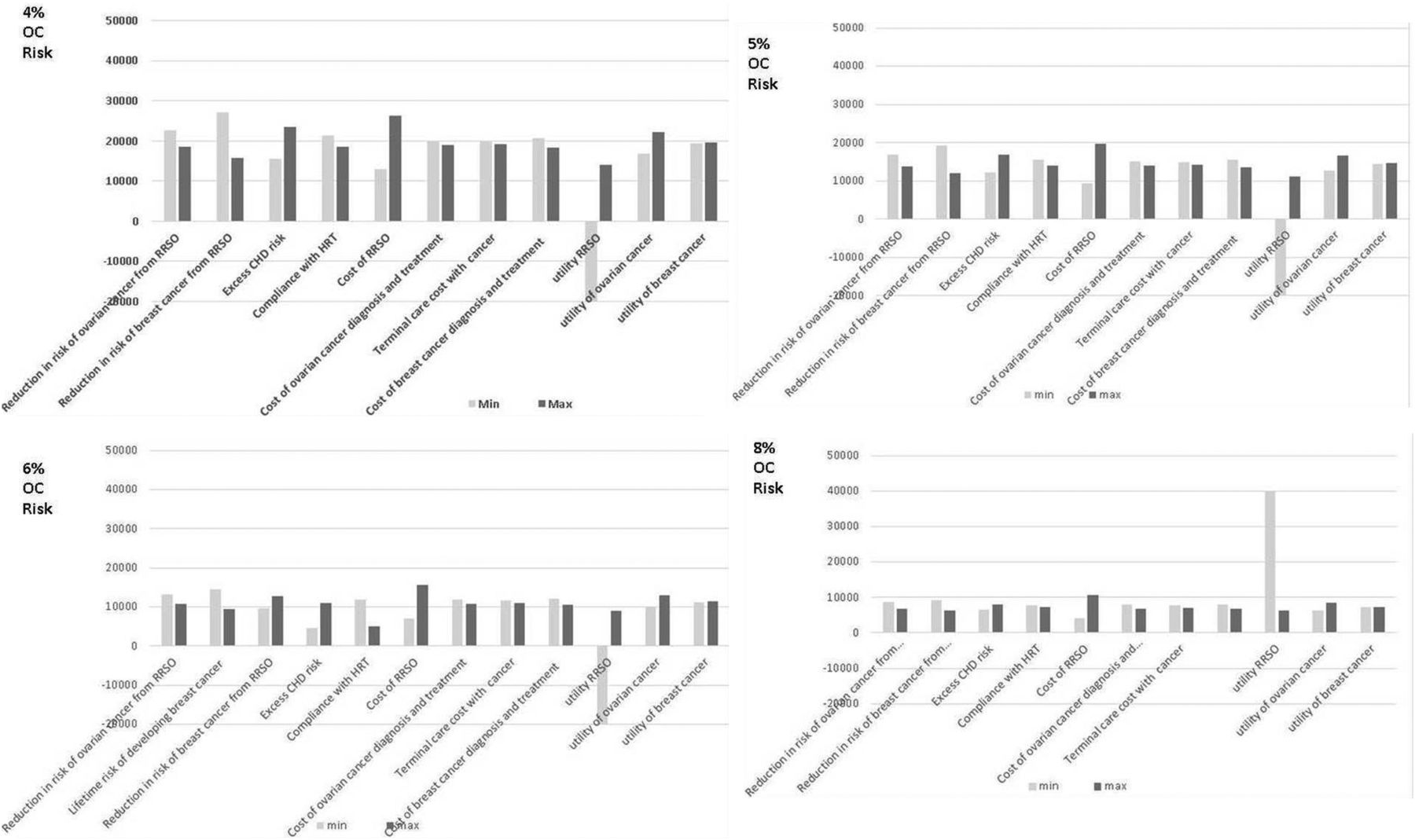
Deterministic sensitivity analysis (figure 2) showed the influence of various parameters on cost-effectiveness falls with a rise in level of lifetime OC risk. Sensitivity analysis indicated model outcomes are not impacted much by various risk probabilities (table 1), costs of surgical prevention or treatment of OC/BC or cardiovascular disease. However, results were sensitive to RRSO utility weights. The one-way sensitivity analysis indicated that the model lacked cost-effectiveness for the lowermost limit of the RRSO utility weight at the 4% OC risk threshold but became cost-effective at the 8.5% risk threshold, with an ICER=£28 532/QALY. Results can also be affected by the HRT compliance rate. If this rate falls beyond the limits of our analysis, the OC risk threshold for cost-effectiveness would rise. If women do not take HRT after RRSO, that is, p6=0, then at OC risk=8.2%, the ICER=£29 071/QALY for 21.8 days increase in life expectancy. This suggests RRSO will be cost-effective at >8.2% OC risk, without HRT. As a scenario analysis, if we assume ‘no reduction’ in BC risk, then RRSO at age ≥40 years is not cost-effective at 4% OC risk but becomes cost-effective at the 6% OC risk threshold (0.13 life-years saved, ICER=£27 212/QALY).

One-way sensitivity analysis for all probabilities, costs and utilities in terms of incremental cost-effectiveness ratio (ICER) of premenopausal risk-reducing salpingo-oophorectomy (RRSO) compared with no RRSO at the different ovarian cancer risk (4%, 5%, 6%, 8%) thresholds. Y-axis: ICER: cost (£) per quality-adjusted life-year (discounted). X-axis: probability, cost and utility parameters in the model. The model is run at both lower and upper values/limits of the 95% CI or range of all probability parameters described in table 1/methods; and both lower and upper values/limits of the cost and utility score parameters given in table 2. Costs are varied by ±30%. ‘Maximum value’ represents outcomes for upper limit and ‘minimum value’ represents outcomes for lower limit of the parameter. CHD, coronary heart disease; HRT, hormone replacement therapy; OC, ovarian cancer.
Figure 3 shows that when all variables are varied simultaneously in a PSA at 2%, 4%, 5%, 6%, 8% and 10% risk thresholds, then 37%, 61%, 74%, 84%, 96% and 99.5% simulations respectively remain cost-effective for the NICE £30 000/QALY ‘willingness-to-pay threshold’ when RRSO is undertaken in premenopausal women. At the NICE threshold of £20 000/QALY, 23%, 46%, 60%, 72%, 91% and 98% simulations will be cost-effective if premenopausal RRSO is undertaken at 2%, 4%, 5%, 6%, 8% and 10% OC risk levels, respectively.

{kind=link}
{kind=link}
{kind=link}
Probabilistic sensitivity analyses cost-effectiveness acceptability curve. Probabilistic sensitivity analysis in which all model parameters/variables are varied simultaneously across their distributions to further explore model uncertainty. X-axis: incremental cost-effectiveness ratio in terms of cost (£s)/quality-adjusted life-year. Y-axis: proportion of simulations. The results of 1000 simulations were plotted on a cost-effectiveness acceptability curve showing the proportion of simulations (Y-axis) that indicated that the intervention was cost-effective at different willingness-to-pay thresholds (X-axis). The first and second dotted lines mark the proportion of simulations found to be cost-effective at the £20 000 and £30000 threshold used by the National Institute for Health and Care Excellence. 37–99% simulations are cost-effective at varying (2–10%) ovarian cancer risk thresholds in this analysis. RRSO, risk-reducing salpingo-oophorectomy.
Discussion
We for the first time precisely define the threshold for lifetime OC risk for recommending ‘premenopausal RRSO’ for OC prevention in the population. Our modelling suggests that RRSO would be extremely cost-effective in premenopausal women ≥40 years with lifetime OC risks ≥4% at the £20 000–30000/QALY WTP threshold44 and equates to >42.7 days gain in life expectancy for an overall ICER=£19 536/QALY. This risk threshold is similar though slightly lower than the recently defined threshold in postmenopausal women.9 This threshold takes into account results of the PSA. Our results are of major significance for clinical practice and risk management in view of declining genetic testing costs and the improvements in estimating an individual's OC risk. With routine clinical testing for certain moderate penetrance genes around the corner and lack of an effective OC screening programme, these findings are timely as it provides evidence supporting a surgical prevention strategy for ‘lower-risk’ (lifetime risk <10%) individuals. Such an approach can contribute to decreasing the number of OC cases and disease burden within the population. This is a key measure needed for moving towards a predictive, preventive, personalised and participatory (P4) medicine stratagem.
A major driver for the cost-effectiveness of premenopausal RRSO has been the beneficial impact on BC risk. Although various initial analyses in the high-risk3 ,47 and low-risk48 populations suggest a reduction in BC risk following premenopausal RRSO, a recent publication49 from a Dutch group found no reduction in risk of BC in BRCA1/2 women and highlighted some methodological limitations of earlier reports.47 ,50 ,51 A key limitation of the Dutch paper is the short 3.2 years follow-up duration. It is likely/plausible that any benefit of decrease in BC cases from early oophorectomy will accrue over a longer period of time. Besides, a subsequent reanalysis (conforming to the Dutch methodology) by authors of the earlier analyses reconfirmed their initially observed reduction in BC risk.52 Our extreme scenario analysis indicates that if there was no reduction in BC risk, RRSO would be cost-effective for higher risk levels for OC of ≥7%.
Model outcomes appear to be very sensitive for the lower limit of utility weight for bilateral salpingo-oophorectomy. Although premenopausal oophorectomy in women is not associated with any difference in generic quality of life, it is reported to be associated with poorer sexual functioning as well as postmenopausal symptoms compared with those who retain their ovaries.53–55 HRT use is essential post RRSO to minimise the detrimental consequences of premature surgical menopause. However, despite HRT, the symptom levels reported (particularly for sexual dysfunction) remain above those who have not undergone premenopausal oophorectomy.56 This limitation needs to be discussed as part of informed consent for the surgical procedure and incorporated into RRSO decision-making process. In addition, we have assumed 80% compliance based on reports from a small study of 521 low-risk women undergoing premature surgical menopause from a single centre. The true compliance in a larger broad-based population sample remains to be established. Hence, premenopausal RRSO should be only offered to women aged >40 years who are committed to taking HRT at OC risk levels >4%. Additionally, longer/more intensive follow-up after RRSO may be needed to address cardiovascular, bone health and psychosexual consequences. Of note, the SD for the utility score in our analysis is large. It is necessary to improve our understanding and precision of RRSO utility scores, particularly in lower-risk women and future research should be directed towards this. Although premenopausal RRSO is undertaken at >35 years for high-penetrance BRCA1/2 carries, the median age of onset for moderate penetrance genes like RAD51C/RAD51D/BRIP1 is higher with no cancers as yet reported at <40 years.14 ,15 Also, 18% of OC in RAD51C/RAD51D carriers15 and 7% OC in BRIP1 carriers14 occur between 40 and 49 years age. Hence, RRSO can be delayed till >40 years in these women.
Our model has numerous strengths and satisfies the several requisites stipulated by NICE for health economic analyses. It includes excess mortality from coronary events described in the literature.7 Besides OC risk, it incorporates impact on BC outcomes and any possible decline in QALYs with the intervention. Other advantages include using QALYs for evaluating health outcomes, using current practice as a comparator, discounting of costs and outcomes by 3.5% and using well-established/proven information from the literature to obtain parameters used in the model.20 The ‘time horizon’ is an important factor in such an analysis.20 This is suitably long enough to reveal any relevant changes in costs and outcomes from our modelling. Only a limited subset of overall costs for OC and BC diagnosis and treatment have been included in the analysis. Additionally, costs for further investigations, management of recurrence or treatment complications were not included. Being conservative in our costs for OC and BC diagnosis and treatment curtails overestimating the advantages of surgical prevention.9
The robustness of our results is enhanced by an extensive sensitivity analyses undertaken. The deterministic one-way sensitivity analysis enabled careful inspection of model outcomes to highlight/ recognise variables that exert greatest influence. The 95% CIs/range of parameters incorporated in the sensitivity analysis are fairly wide. This further adds to the rigour of the results. It is reassuring that despite probabilities varying widely the model remains largely cost-effective. That 30% variation in costs did not significantly affect outcomes indicates that costs of surgical prevention or treatment costs for OC/BC/cardiovascular events do not have much significance in affecting modelling outcomes. We undertook both PSA and DSA in line with recommendation from authorities like NICE.20 PSA adds rigour by facilitating all parameter probabilities to be varied concurrently in order to properly characterise model uncertainties and any impact on final outcomes. The cost-effectiveness of ≥61–74% of PSA simulations at ≥4–5% OC risk reconfirms that premenopausal RRSO for OC prevention is beneficial in health economic terms at these risk thresholds.
The exclusion of increased mortality from lung/colorectal cancer found in the Nurses Health cohort may be considered a weakness of our analysis.7 However, these additional deaths from cancer that were observed could have been confounded by smoking or other risk-related behaviours. Much larger cohort studies have shown smoking per se is linked to menopause,57 ,58 and after stratification by smoking, any increase in lung cancer risk reported following oophorectomy is limited to those who smoke.57 Furthermore, the EPIC study (337 802 women) reported lack of any significant association of colorectal cancer risk with age or surgical menopause.59 Even if we do include the impact of all-cause mortality (1:8) found in the Nurses Health Study in our model, the model remains cost-effective at an OC risk ≥7% (ICER=£29 128/QALY, 0.1 life-years gained). We did not account for complications from RRSO in our analysis, which have been reported to occur in 1.5–5% of high-risk women.60–62 This is an important part of preoperative surgical consent by the treating clinician and built into the decision-making process.
Our findings indicate that RRSO would be cost-effective even for women with (a) mutations in moderate risk genes like RAD51C,11 RAD51D,12 BRIP1;13 (b) BRCA1/BRCA2-negative women from high-risk families; and (c) those who have an FDR with OC. We have shown that ∼75% of OC familial relative risk is not accounted for by BRCA1/BRCA2 mutations10 and that if all OC susceptibility alleles are identified then 53% of all OC occur in 8.8% of the population with ≥5% risk and 62.8% OC occur in 13.4% of the population at >4% risk.18 Unlike earlier models (BOADICEA,63 BRCAPRO64) that underestimate OC risks in BRCA1/BRCA2-negative women, a recently published model incorporates the effects of an observed ‘polygenic risk score’ (PRS), which incorporates all known common genetic variants leading to more accurate risk prediction in BRCA1/BRCA2-negative women. For example, the lifetime risk of OC in a woman who has two affected FDRs and is found to test negative for a BRCA1/2 mutation is >5% if her PRS score is in the upper half of the PRS distribution.18
The shifting landscape resulting from new genetic discoveries, better risk estimation and rapidly changing genetic testing technology has important implications and offers opportunities for cancer risk management and prevention. SNP profiles in combination with family history18 data and other epidemiological risk factors65 provide the ability to discriminate between low (1–2%) and intermediate (>3% to <10%) OC risk individuals and have an increasingly important role to play in personalised OC risk prediction, with implications for OC prevention. Our findings have significant implications for changing practice and guiding policy for developing a surgical prevention strategy for OC. This fits well with the newly published Independent Cancer Task Force, Cancer Strategy for England 2015–2020,66 which highlights the need for major emphasis and focus on cancer prevention as well as the Obama Precision Medicine initiative.67 The significance and need for fresher/novel cost-effective targeted prevention strategies is further heightened by the challenging economic environment, increasing costs of healthcare, as well as rising prices of new OC drugs/treatment strategies. However, implementation of this approach requires building knowledge, understanding and awareness among health professionals and laypeople through education, dissemination of information, as well as media campaigns, which in turn are associated with additional costs. Given the many side effects of premature menopause, it also requires women to understand the need to take HRT till the age of natural menopause. Additionally, research needs to be directed towards understanding the acceptability, uptake and impact of genetic testing, risk prediction and RRSO at lower-risk thresholds in the general population. Furthermore, care commissioners, general practitioners, genetics teams and gynaecologists need to develop additional downstream care pathways for these at-risk women for this approach to be successful.
References
Supplementary materials
Press release
Files in this Data Supplement:
Footnotes
Contributors RM, UM and RL developed original concept and design of the study. RM, RL and UM developed the model. All authors were involved in the design of the work, and data interpretation of the health economic and statistical analysis. RM, RL and VD did the health economic analysis and prepared the tables and figures. RM and RL prepared the first draft of the manuscript and all authors contributed to subsequent drafts. All authors critically contributed to and revised the manuscript and approved the final version. All authors had full access to all of the data (including statistical reports and tables) in the study and can take responsibility for the integrity of the data and the accuracy of the data analysis.
Acknowledgment The study was supported by researchers at the National Institute for Health Research University College London Hospitals Biomedical Research Centre.
Funding The study is not funded by any charity or grant.
Competing interests UM declares a financial interest in Abcodia, which has an interest in ovarian cancer screening and biomarkers for screening and risk prediction.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data available.