Article Text

Abstract
Smith-Magenis syndrome (SMS) is a clinically recognisable contiguous gene syndrome ascribed to interstitial deletions of chromosome 17p11.2. Patients have a phase shift of their circadian rhythm of melatonin with a paradoxical diurnal secretion of the hormone. Serum melatonin levels and day-night behaviour were studied in nine SMS children (aged 4 to 17 years) given acebutolol, a selective β1-adrenergic antagonist (10 mg/kg early in the morning). Cardiac examination, serum melatonin, motor activity recordings, and sleep diaries were monitored before and after drug administration. The present study shows that a single morning dose of acebutolol suppressed the inappropriate secretion of melatonin in SMS. A significant improvement of inappropriate behaviour with increased concentration, delayed sleep onset, increased hours of sleep, and delayed waking were also noted. These results suggest that β1-adrenergic antagonists help to manage hyperactivity, enhance cognitive performance, and reduce sleep disorders in SMS.
- Smith-Magenis syndrome
- circadian rhythms
- melatonin
Statistics from Altmetric.com
First described by Smith et al 1 in 1982, the Smith-Magenis syndrome (SMS) is a contiguous gene syndrome resulting from interstitial deletions of chromosome 17p11.2 (incidence 1 in 25 000 births1 2). Clinical features include craniofacial anomalies, mild dysmorphism, short stature, brachydactyly, developmental delay, and abnormal behaviour.3-5 Behavioural problems include hyperactivity, attention deficit, self-injury, tantrums, and sleep disturbance. These symptoms have a major impact on the children and their families. The diagnosis is based on high resolution karyotype and fluorescence in situ hybridisation (FISH).6
The specific sleep disturbance has been previously described7 and includes early sleep onset, frequent awakenings, and early waking. Moreover, “sleep attacks” at the end of the day are consistent features of the disease and should be regarded as highly specific diagnostic criteria in SMS. Taken together, these features support the view that SMS patients have a sleep phase advance.
Melatonin, the main hormone of the pineal gland with light-dark cycles, is normally secreted during the night. Interestingly, all SMS patients have a phase shift of their circadian rhythm of melatonin, with diurnal secretion of the hormone.8-10 Tantrums and tiredness occur when melatonin rises and children have naps and sleep attacks when melatonin peaks at midday and in the evening, respectively.9 Considering that the behavioural problems may be correlated with the inverted circadian rhythm of melatonin and night sleep insufficiency in SMS, we hypothesised that at least some of the hyperactivity and attention deficit might occur because the patients struggle against sleep when melatonin rises during the day. Because the circadian rhythm of melatonin is controlled by the sympathetic nervous system, and the synthesis and release of melatonin are stimulated by noradrenaline via β1-adrenoreceptors,11 12 nine SMS children were given acebutolol, especially as β1-adrenergic antagonists have been previously shown to reduce the production of melatonin.13 14 Here, we report on the suppression of the inappropriate diurnal secretion of melatonin and the significant improvement of sleep disorders in SMS children given acebutolol.
Methods
PATIENTS
Nine children (five boys, four girls, aged 4-17 years) were recruited from the cohort of SMS children diagnosed at Necker-Enfants Malades Hospital. The bioethical human research committee approved the investigation protocol and the parents signed an informed consent form before inclusion in the study. All SMS patients met the clinical inclusion criteria, namely facial dysmorphism, developmental delay, hyperactivity, attention deficit, and sleep disturbances (fig 1). All carried a 17p11.2 deletion confirmed by FISH analysis using an ONCOR probe (D17S258) (fig 1). All treatment was discontinued two weeks before inclusion and patients received no drugs or melatonin in the course of the study.

(A) FISH analysis in SMS. (B) Facial appearance of a SMS child. (C) Melatonin secretion is under the control of photic information transmitted from the retina through the suprachiasmatic nuclei of the hypothalamus and sympathetic nervous system.(D) Inversion of serum melatonin rhythm in SMS (solid lines) compared to age matched controls (dotted lines).
PROCEDURES
The patient's sleep/wake schedules were investigated before and after two and six months of drug administration during consultations with the same investigator (HDL). Sleep and day diaries were filled in at home by the parents over a period of one month. For ambulatory actigraphy (nine patients), recordings were made during one minute periods using the Actiwatch score (Cambridge Neurotechnology). Outpatient actigraphy data were collected over a 11-28 day period before and after drug administration. Actigraphy data were analysed for average activity offset and onset, using the Actiwatch software programs.
The children were admitted for 48 hours between May and September 2000 to our paediatric cardiology unit for investigations and plasma melatonin monitoring. Cardiac examination, ECG, and heart ultrasound were conducted before drug administration and a 48 hour cardiac holter recording was conducted during hospitalisation. It is important to note that three children had cardiac disorders, namely transposition of the great vessels with septal defect and pulmonary stenosis, operated on at birth (one case), ventricular septal defect (one case), and cardiac rhythm disorder and ventricular extrasystoles (one case). These cardiac anomalies did not preclude β1-adrenergic antagonist administration. None of them had asthma or respiratory disorder. Pulse rate, blood pressure, and temperature were measured every two hours. Blood samples were drawn from an indwelling forearm catheter every two hours, from 10 am on day 1 to 10 am on day 3 (two days, two nights). Samples were transferred to heparinised plastic tubes, centrifuged, and frozen at –20° until assay.
Melatonin was measured using a commercially available radioimmunoassay kit (melatonin direct RIA, IBL Hamburg). The minimal detection level of the test was 3.5 pg/ml. The intra-assay coefficient of variation for control samples was 8% and the corresponding inter-assay coefficient of variation was 14.9%. Previous studies have described the level of plasma melatonin in age matched controls.9 15 Starting on the second day of admission, patients received a single oral dose of acebutolol at 8 am (10 mg/kg). The treatment was continued at home for up to six months, at the same dose, taken every morning at breakfast time.
STATISTICAL ANALYSIS
Significance of differences was calculated using the Studentt paired test. A p value of <0.05 was considered to be statistically significant.
Results
Monitoring endogenous plasma melatonin supported the phase shift and protracted duration of melatonin secretion in SMS children (fig 1). A broad range of endogenous melatonin levels was observed in SMS, as previously described in healthy children.16 Indeed, mean diurnal melatonin levels (10 am-8 pm) ranged from 5 to 157 pg/ml, irrespective of the age and sex of the children. All SMS children had lower melatonin levels during the night than during the day (mean nocturnal values 25 pg/ml, 10 pm-8 am, table 1). After a single drug administration, plasma melatonin levels rapidly decreased in all SMS children (table 1, fig 2), the mean melatonin levels falling from 68 pg/ml to 8 pg/ml after drug administration. Individual melatonin levels decreased 3-20 fold, remained low from 8 am to 6 am the next day, and rose again from 6 am to 8 am before drug administration (fig 2). No desensitisation was observed over the two month period of drug administration in three children (not shown).
Plasma melatonin before and after treatment

Circadian variation of plasma melatonin in Smith-Magenis syndrome before and after administration of β1-adrenergic antagonists. Blood samples were drawn every two hours over 48 hours in patients aged 15 years (A), 8-9 years (B, C, D), 7 years (E), and 4 years (F). Acebutolol was given at 8 am on the second day.
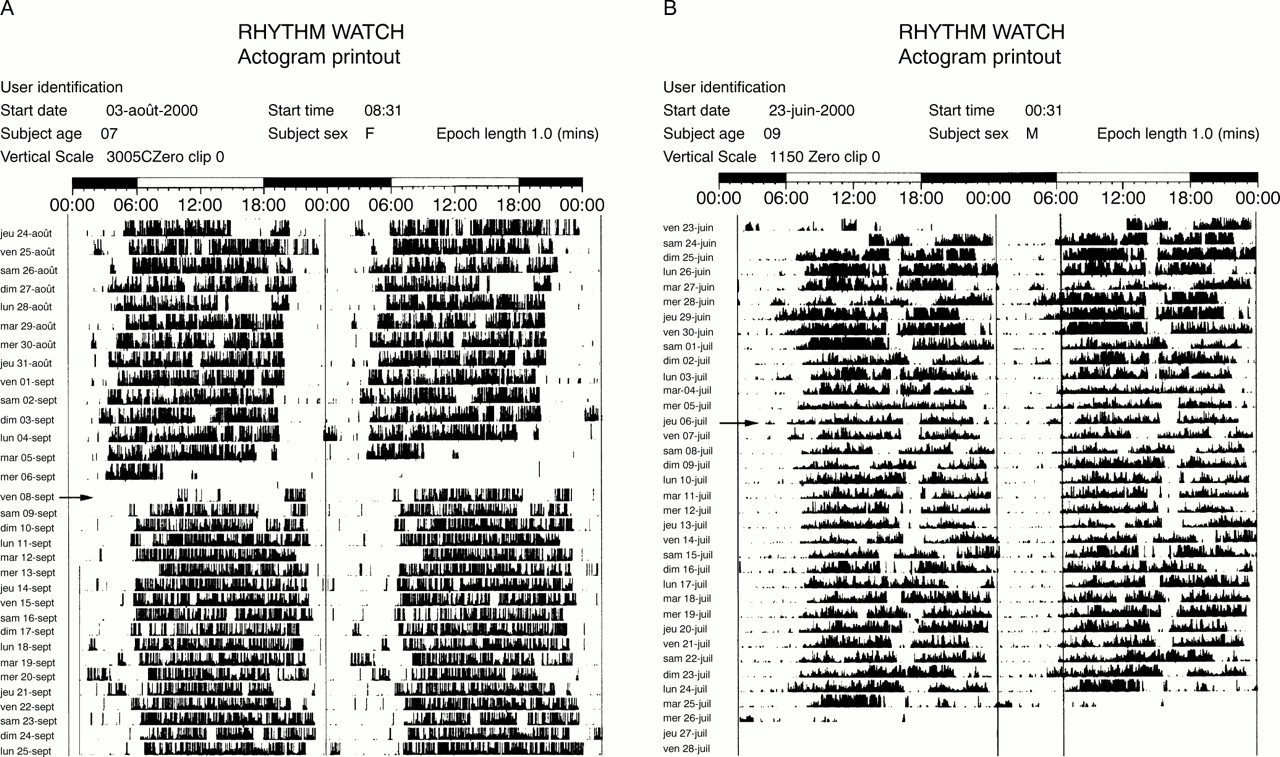
β1-adrenergic antagonist administration resulted in a major improvement of sleep disorders. Indeed, before drug administration, mean sleep onset was 9.15 pm (range 8.30-10 pm), mean waking was 5.40 am (range 4-7 am), and mean duration of sleep was 8.20 hours (range 7.15-9 hours, table 2). Actigraphy data showed that night parameters dramatically improved in children given acebutolol (fig 3). In fact, mean sleep onset was delayed to 9.40 pm (range 8.45-10.30 pm), mean waking to 6.40 am (range 5-7.30 am), and mean duration of sleep to 9 hours in SMS children given acebutolol (range 8.15-10 hours) (table2). Consequently, day behaviour based on diaries (filled in by the parents and school teachers) and questionnaires (filled in during consultation) markedly improved. While untreated children had one to three naps per day and frequent sleep attacks at the end of the day, acebutolol administration resulted in the disappearance of naps and sleep attacks (except for the youngest child who had one nap at midday). Children only fell asleep during car drives. The explosive tantrums (one to two each day) were less frequent (one or two per week) and could be easily managed. Parents, teachers, friends, and uninformed neighbours noted more appropriate behaviour, especially outside the family.
Effects of β1-adrenergic antagonist on sleep/wake patterns in SMS (Actiwatch)

{kind=link}
{kind=link}
{kind=link}
Actigraph of a 7 year old girl (A) and 9 year old boy (B) before and after acebutolol administration (arrow). Note decreased motor activity following drug administration in patient B.
Before treatment, SMS children had poor concentration (less than 10 minutes, even for the oldest), while they could concentrate for 30-60 minutes or more for games, puzzles, gardening, or little jobs at home when given acebutolol. One of them could look at a book quietly, which had never occurred before. Another child could do his homework after school with his mother. Teachers acknowledged better concentration during school time and the children were reported to be quieter and less hyperactive (fig 3). Home and social behaviour improved but remained problematical. No significant increase of cognitive performance was observed. Finally, no side effects of β1-adrenergic antagonists were noted and all parents asked for continuation of acebutolol at the end of the trial.
Discussion
We have hypothesised that behavioural problems, hyperactivity, and attention deficit could be related to sleep deprivation and inappropriate diurnal melatonin release in SMS. Here we show that β1-adrenergic antagonist administration suppressed the inappropriate diurnal secretion of melatonin in Smith-Magenis syndrome. Acebutolol decreased motor hyperactivity, reduced naps and sleep attacks during the day, and controlled outbursts, which were shorter and less frequent. Attention improved and interpersonal interactions were less confrontational as parents and teachers did not have to work as hard to control the children.
Sleep patterns consistently improved in all children given β1-adrenergic antagonists. All nine patients had fewer naps and tantrums and actigraphy data showed a significant improvement of their night parameters. Mean sleep onset was delayed by 25 minutes, waking by 60 minutes, and the mean gain of sleep was 40 minutes. Participation of the child in family life, which was hampered by fatigue and sleepiness, was markedly improved by acebutolol administration. However, sleep awakenings persisted in most cases, especially in the young children, and waking time remained early.
β1-adrenergic antagonists are largely used in the management of hypertension, arrythmias, and migraine in children17-19 and were particularly well tolerated with no side effects in SMS. β1-adrenergic antagonists have been previously shown to reduce nocturnal plasma melatonin, the main hormone of the pineal gland.20 Photic information is transmitted from the retina to the pineal gland through the suprachiasmatic nuclei of the hypothalamus and the sympathetic nervous system.12 21 Normally, at twilight, the photoreceptors release noradrenaline, thereby enhancing the number of α1- and β1-adrenergic receptors in the pineal gland and activating the N-acetyltransferase which triggers the synthesis and release of melatonin. The abnormal circadian rhythm of melatonin in SMS and its relationship with chromosome 17 deletion remain unclear. It may result from an alteration of the input/output signalling pathway, for example, photic stimulation in the retina/retinohypothalamic tract, an alteration of the circadian time keeping system (clock genes) of the suprachiasmatic nuclei, or an abnormal transmission from suprachiasmatic nuclei to an output signalling pathway of postganglionic fibres ascending to the pineal gland.22 How melatonin acts on sleep is also unknown. Melatonin may modify brain levels of monoamine transmitters, thereby initiating a cascade of events culminating in the activation of sleep.23 24
Neurologically disabled and mentally retarded children frequently exhibit disrupted sleep-wake cycles and severe sleep disturbances.25 26 The use of melatonin at the end of the day has been recently suggested for the treatment of chronic sleep disorders in disabled children.27-29 Yet, while its kinetics are erratic, the amount of hormone released remains normal in SMS. Thus, its inappropriate secretion should be corrected before exogenous hormone administration.
In conclusion, our results indicate that β1-adrenergic antagonists suppressed the inappropriate diurnal melatonin secretion and improved sleep and behavioural disorders in SMS. Ongoing trials using various β1-adrenergic antagonists, with different half life kinetics, combined with evening melatonin administration30 will, it is hoped, restore the physiological circadian rhythm of melatonin in Smith-Magenis syndrome.
Acknowledgments
We are grateful to the children, parents, and the ASM 17 family support group of France for participating in this study, and to Pierre Frotte, David Genevieve, and M C Nollen for helpful cooperation. Part of this study was supported by Institut de Recherche Internationnales Servier.