Article Text

Abstract
A family history of breast cancer has long been recognised as a significant risk factor for breast cancer. Quantifying that risk has been approached in publications and practically in a number of different ways. Increasingly regional genetics departments are called upon to help clarify guidelines for referral of women with a family history of breast cancer for genetic testing and to clarify breast cancer risk for women seeking early mammographic screening. This paper represents the current consensus guidelines from the UK Cancer Family Study Group and discusses some of the difficulties surrounding genetic risk estimation.
- guidelines
- genetic risk
- breast cancer
Statistics from Altmetric.com
Cancer genetics is a new and rapidly expanding speciality to which clinicians come with expertise in clinical and molecular genetics and in oncology. Most such specialists are based in the Regional Clinical Genetics Department. One of the main reasons for referral (expanding rapidly over recent years) is a family history of breast cancer. Women with a family history of breast cancer are usually seen initially by the primary care team and referred to either a symptomatic breast clinic, to a familial breast cancer clinic, or directly to the clinical genetics service. Breast screening policies in such women vary widely across the country, particularly with regard to level of risk at which screening is deemed appropriate, the age at first screen, screening interval, type of screening, route of access to screening or genetics clinics, and the collection of outcome data.
These guidelines have been developed to help clinicians at primary care level and at the district breast clinic to decide when it is appropriate to reassure patients concerned about genetic risk of breast cancer if the genetic risk is low, when early breast screening might be appropriate, and when, in addition, to refer to a specialist genetics clinic for further assessment and investigation. They are intended as guidance regarding genetic predisposition only and do not take epidemiological risk factors into account.
The Cancer Family Study Group (CFSG)
The CFSG was set up in 1981 by a group of oncologists, scientists, and geneticists interested in hereditary cancer predisposition. It has become the main forum for research collaborations and education in the field of cancer genetics within the UK. Since its initial inception there has been an explosion of new discoveries in cancer genetics and the membership has escalated; official members now number around 250 with representatives from all the regional genetics centres. Currently the membership comprises a wide spectrum including specialist nurses and psychologists as well as basic scientists and clinicians from all specialities with an interest in this relatively new area of medicine. There are representatives from general practice, surgery, radiology, radiotherapy, and oncology as well as genetics. There is a steering committee of 11 elected members and a representative from the Cancer Research Campaign and the Imperial Cancer Research Fund who have partially funded this organisation since its inception; other funding has been provided by the MRC. The UKCFSG meet twice a year to discuss new research proposals, to debate guidelines, to give feedback on research progress, and to present new data and updates on clinical management issues. These guidelines have been presented to and commented on by the membership at these meetings over the past three years and the manuscript has been scrutinised by the steering committee.
The guidelines (table 1)
These guidelines are preliminary and are likely to change as new information comes forward. They are particularly pertinent to the UK health care system and clinicians need to be familiar with what facilities are available locally and how to access these, as this at present varies across the country. For example, few regions in the UK have at present the facility to recall women for mammography outside the National Health Service Breast Screening Programme (NHS BSP) and there is in general no specific funding allocated to breast screening in women under 50 years with an increased genetic risk of breast cancer. Where breast unit screening clinics are not established, breast screening tends to be somewhat ad hoc and audit of the outcome of screening activity for a large cohort of women is impossible. Screening in these circumstances is unsatisfactory since at present the evidence for any mortality benefit in high genetic risk women is lacking. A recent report of a Working Group for the Chief Medical Officer (distributed to the UK NHS for information)1 recommended that family history clinics without the facility to audit activity and outcome should not be funded. It also recommended that management of moderate risk level women should fall within the remit of the Specialist Calman Breast Units working to guidelines agreed between the breast units and the Regional Cancer Genetics Centre, and that units setting up a service without specialist genetic input should not be funded. In these guidelines we endorse the proposed model and suggest that asymptomatic women at low genetic risk are dealt with at primary care level with reassurance, those at moderate genetic risk are evaluated and screened at breast unit level (resources permitting), and high risk women are assessed further by the regional genetics service.
Guidelines for referral and screening mammography with one, two, or three relatives affected with breast cancer at various ages
Resources are the main concern where funding is not in place. Although some purchasers have committed funding to the molecular analysis of cancer predisposing genes and the clinical cancer genetics services, many others have not and funding for the cancer genetics staff within the genetics service is also very variable. At district level, no mammographic screening is funded for women under the age of 50 within the NHS Breast Screening Programme; on the whole this is arranged via the symptomatic service and puts an additional burden on radiology services and busy breast clinics. Collection of data on breast cancer risks and screening outcomes in this group may be most effectively coordinated on a regional basis and could be collated by the cancer genetics service, although the screening and clinical review of patients is most appropriately carried out in the local breast unit. Funding for data collection and audit must be provided if monitoring the outcome of screening activities in this setting is to be successful. The cancer geneticist should have an input in the multidisciplinary approach to breast cancer management.
Risk assessment
Until firm evidence accrues of a mortality benefit in the high risk group of women, it is impossible to present definitive guidelines about how to screen women and where to draw the line above which women are deemed to have an increased genetic risk for breast cancer. It is relatively easy to calculate the genetic risk that a breast cancer will develop in any woman given her family history of the disease. Segregation analysis is a technique used to model disease inheritance in populations. It provides a mathematical description of a genetic model reflecting the most likely pattern of inheritance of a disease in a given population. It reflects the average gene frequency and penetrance for familial clustering. The models most commonly used for estimation of genetic breast cancer risk use a general model rather than a gene specific model. The estimates for gene frequency and age related penetrance (breast cancer risk for a gene carrier) are therefore necessarily general. Published segregation analyses for breast cancer mostly predict autosomal dominant inheritance with low gene frequency and high penetrance.2 3 IfBRCA1 and BRCA2gene carriers are identified and removed from a cohort of women with a family history of breast cancer, there is still a residual genetic risk from unidentified genes.4 The estimated residual genetic risk is lower than predicted by whole population analysis because the effect of the higher risk genes has been removed. Where genetic status is known, gene specific parameters are more appropriate.5 6 In all models and methods there are inherent inaccuracies because of uncertainties about key inputs.6
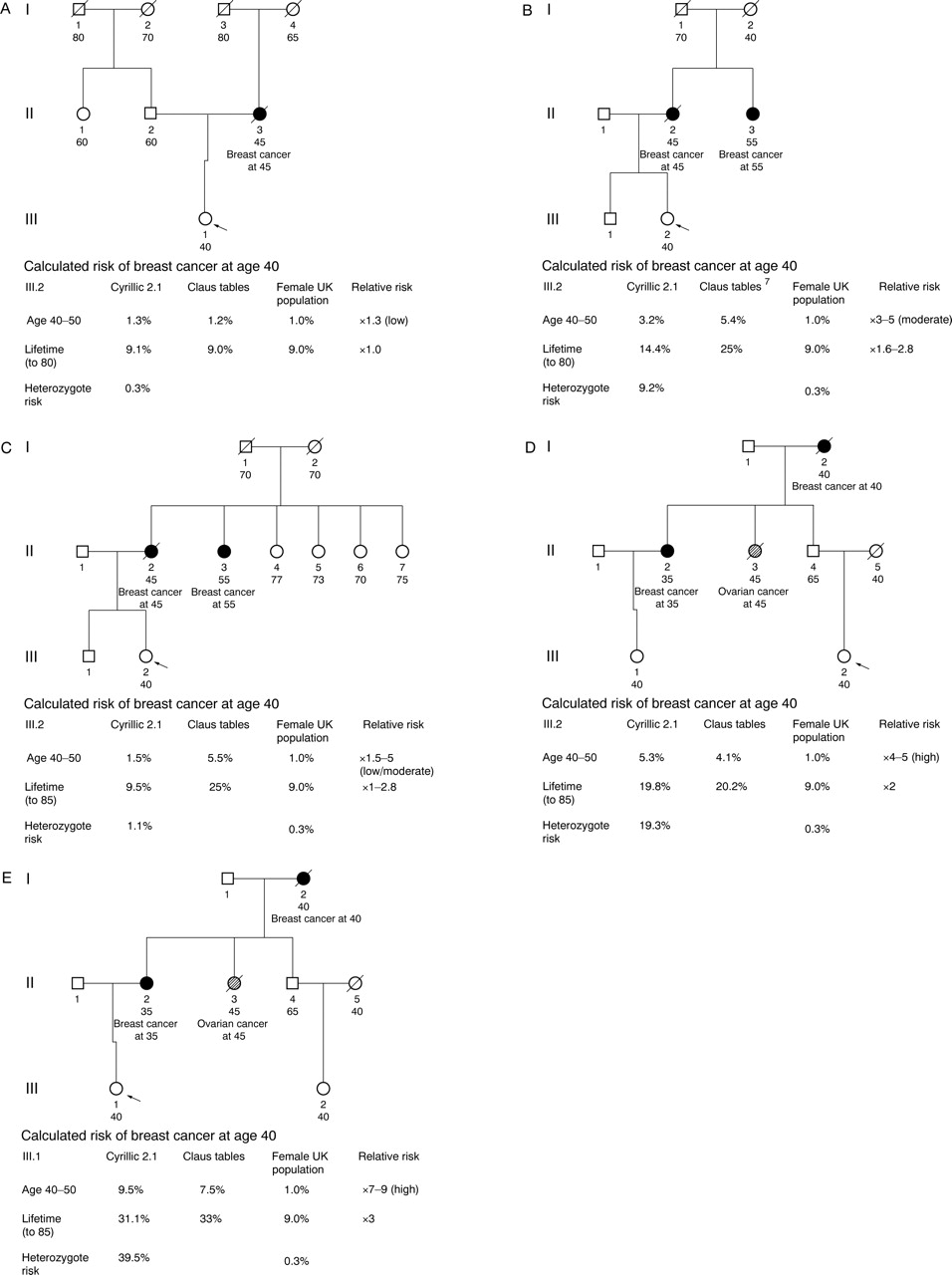
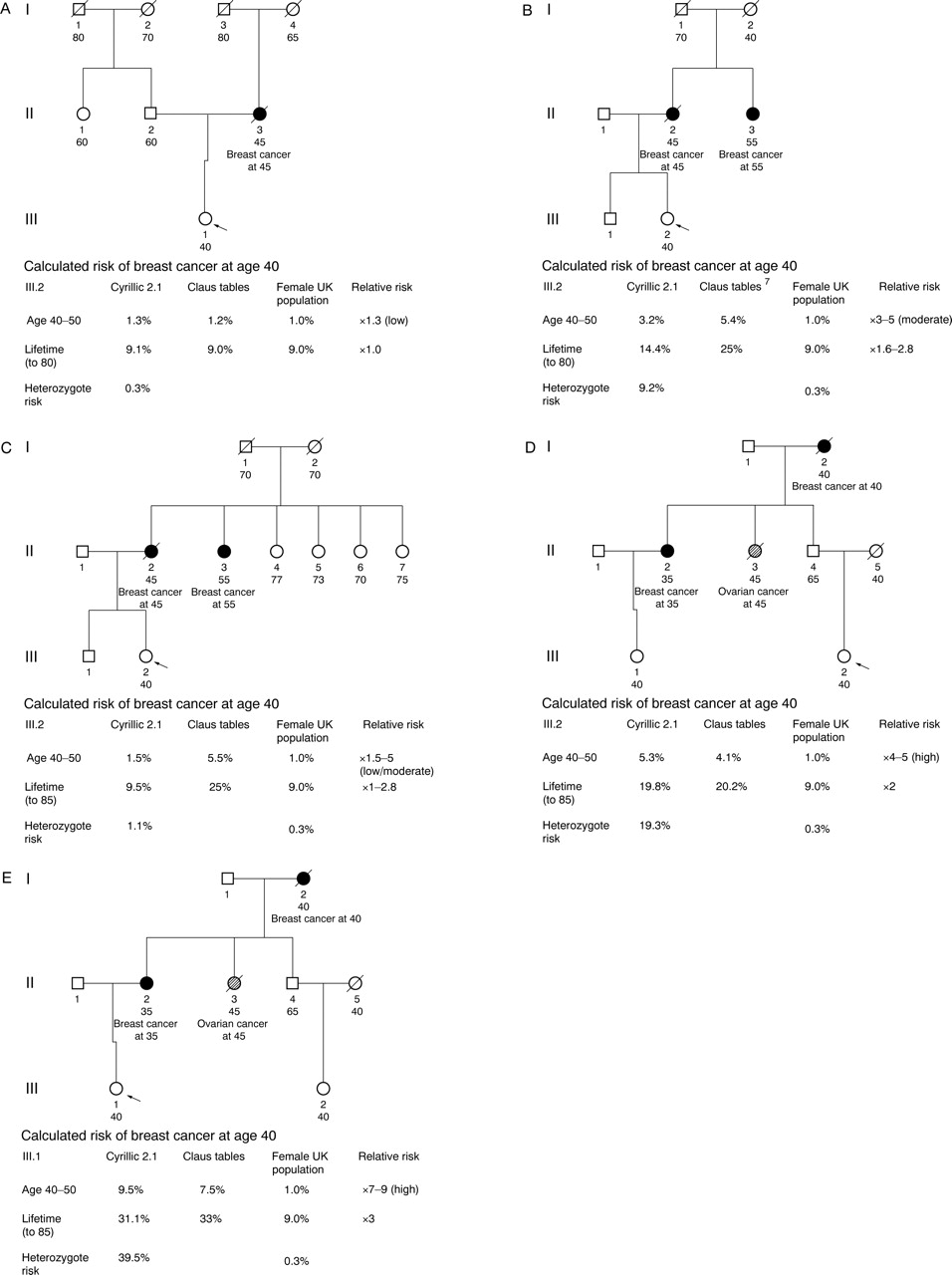
Bearing these factors in mind, parameters from a segregation analysis2 3 can be used to calculate genetic breast cancer risk for any specified time period.7 Parameters from a segregation analysis using data from the Cancer and Steroid Hormone Study (CASH)2 are commonly used for genetic risk estimation and form the basis of risk calculations in both the published and clinically useful risk tables7 and the commercially available computer software Cyrillic 2.1 published by Cherwell Scientific. Data for very early onset breast cancer are under-represented in the CASH data and this cohort was selected for breast cancer cases with age at onset under 55 years, leading to another potential source of uncertainty in this model. A risk calculation based on these data (using Cyrillic 2.1) is illustrated in fig 1 for a 40 year old woman with various levels of risk (table 1, fig1A-E). The Claus tables7 give risks based purely on affected subjects without accounting for unaffected family members, so give a higher risk than the whole pedigree based method, but nevertheless with a very simple pedigree this effect is not great (fig1A, B). The risk modifying effect of many unaffected relatives, however, can be seen in the pedigree in fig 1C and this cannot be taken into account using the Claus tables. This is also a problem in the case of small families or adopted parents, for example, where the risk estimation could be very misleading in either direction when more information becomes available. Here, the woman concerned about her risk may be reassured by the effect of her own age; as her own age increases she becomes statistically less likely to be a carrier of a high risk gene and therefore the risk to her offspring falls. A strong paternal family history can also confer a significant risk which cannot be assessed using the Claus tables (fig 1D). Ovarian cancer is 10 times less common in the general population than breast cancer and ovarian cancer occurs in many families found to haveBRCA1 and BRCA2mutations. Thus, ovarian cancer in a breast cancer family increases the chance of a genetic predisposition (fig 1E).
{kind=link}
Risk calculation in low (A) and moderate (B) risk patterns. Moderate risk modified to low by unaffected female relatives (C). Risk because of strong paternal family history (D) and high risk (E) family history. The annotation indicates the age related actual and relative risks in each situation compared with the UK Office of Population Census and Surveys data on breast cancer incidence for the UK. Both risk estimation methods illustrated use a purely genetic model and do not take epidemiological risk factors into account, so may significantly underestimate risk in low and moderate risk women, in particular where there are high risk life style factors.
Although the risk figures given in the tables and by the computer programme appear very precise, this reflects the fact that they are generated by a mathematical calculation; the illustrations give some idea of the variation possible depending on the data and the method used. Absolute risks may not be particularly helpful (especially if these are incorrectly assessed owing to the problems associated with any risk estimation method currently available). High risk subjects in particular should be reviewed by a clinician with expertise in cancer genetics and risk analysis before clearly categorising them as high risk. This should be available before any major clinical decisions are made including, in particular, genetic testing and prophylactic surgery. The risk estimation methods outlined here are merely a means of categorising people fairly into genetic risk groups.
It is not clear how conventional epidemiological risk factors can best be included as a modifier of risk. However, some methods have attempted to investigate what effect such factors might have.8 9There are mathematical models published which incorporate these factors10 11; different models may be better used in different circumstances. Models such as the Gail model take epidemiological risk factors into account but underestimate the genetic risk where this is significant. Thus, predictions using the Gail model may be more accurate for women with a low component of genetic risk; for women with a high genetic risk there are as yet no clear data which allow incorporation of conventional epidemiological risk factors into a general genetic model.
The various methods of risk estimation need to be validated in prospective studies but for the time being can provide a useful means of standardising risk estimation and selecting only women at moderate or high genetic risk for breast screening studies.
Initial assessment of the family history and reassurance of low risk subjects should take place at primary care level and these guidelines provide some indication of where reassurance is appropriate. Fig 1A-E gives examples of risk estimation for women with a family history of breast cancer at low risk (<3 times the age related risk) (fig 1A, C), moderate risk (3-4 times the age related risk) (fig 1B), and high risk (>4 times the age related risk) (fig 1E). Unaffected female relatives on the same side of the family as affected relatives are important in reducing risk of a strong genetic predisposition, and a history that initially appears moderate or high risk on further assessment may become lower risk (fig 1B, C). Except in the highest risk groups, a woman remaining unaffected in her fifties will have sufficient reduction in genetic risk in many cases to return to the lower risk category, as the population risk rises and her risk becomes less than three times the age related risk.
An accurate risk assessment and the outcome of clinical examination and mammography should be recorded in each screened woman to facilitate audit. Clinical trials of chemoprevention may be an appropriate option for some women, since few of these will be eligible for genetic testing at present.11 12
The genetics clinic
RISK ASSESSMENT
For patients where the chances of the family history being the result of a high risk gene are strong (therefore those in the highest risk category), referral to the genetics clinic for further assessment is appropriate. The genetics team can undertake detailed family studies initially by constructing a complete family tree and verifying key data. Using these data, a modified genetic risk can be estimated. Subjects referred to the genetics clinics need to be informed that molecular genetic testing may not be possible in every case. In many cases, there are no suitable DNA samples available from affected family members, in others detailed scrutiny of the family history and investigation to confirm diagnoses may indicate a lower chance of a genetic predisposition than originally thought. In addition, some women elect not to have genetic testing and before testing it is imperative that the person has an understanding of the limitations and potential disbenefits of genetic testing in addition to any potential benefits.13
Molecular genetic diagnostic testing (particularly presymptomatic testing) should only be carried out by the clinical genetics service using a quality assured diagnostic laboratory. However, even where genetic testing is not possible, many women will be eligible for studies in chemoprevention and screening which can be coordinated either by the genetics team or the breast unit or preferably by both in collaboration. In addition, these families may be suitable for genetic research to identify other breast cancer predisposition genes. Quantification of a person's risk (often lower than they thought)14 and information about screening and clinical trials is usually helpful both to the patient and the referring doctor, and the level at which this is provided varies at present across the country depending on local resources and interests. Appropriate collaboration with the regional cancer genetics specialist will ensure referral of appropriate cases for formal genetics assessment within the regional genetics service. Women need information about level of risk and risk management options in order to make informed choices about their own health care. Current evidence indicates that risk counselling does improve knowledge and is not associated with increased anxiety.15 16
OVARIAN CANCER
A discussion reviewing the likelihood of a genetic predisposition to breast cancer on the basis of the family tree may incorporate concerns about ovarian cancer risk. A family history of young breast cancer and ovarian cancer is more likely to be because ofBRCA1 than a history of just breast cancer. Whether a causative mutation is detected or not, ovarian cancer may be a significant risk to a gene carrier or a woman at risk of carrying the gene. In the UK, data on the outcome of ovarian screening for women with at least a 1 in 15 lifetime chance of developing ovarian cancer is collected as part of a national study. Outside this framework, ovarian screening may or may not be offered depending on local interests and availability, but at present there is no evidence of any survival benefit from current methods of ovarian screening. For a woman with even a strong family history of breast cancer (three or more under 60 years of age), more than 60% are not the result of a detectableBRCA1 mutation. Raising concerns about ovarian cancer risk may then not be appropriate; however, opinions and practices vary and there is no consensus as yet. In general, the UKCFSG would prefer ovarian screening to be offered only as part of clinical trials. Where ovarian cancer risk is deemed sufficiently increased, any discussion of screening must include a discussion of the option for prophylactic oophorectomy.
MANAGEMENT OF BREAST CANCER RISK
Again the options are screening aimed at early detection, chemoprevention (Tamoxifen is not yet licensed as a chemopreventive agent in the UK but chemoprevention trials continue), and prophylactic surgery (for very high risk patients). These options can be discussed in detail at the genetics clinic.
PSYCHOLOGICAL SUPPORT
The provision of professional psychological support for cancer patients is patchy in the UK so the only genetics units with such support tend to be those where a specific psycho-oncological research group is involved in collaborative research. Access to psychological assessment and support locally is helpful and in some cases may be essential (for example, women considering prophylactic mastectomy).
MOLECULAR TESTING
Currently, in the UK, an unaffected woman from a breast cancer family could not have an immediate genetic test. In the relatively rare families where a specific gene mutation has been identified in an affected family member, presymptomatic testing can be offered. In certain ethnic groups where specific mutations are common, the absence of a mutation in an “at risk” woman significantly reduces her breast cancer risk (for example, Ashkenazim17-19). Analysis of theBRCA1 and BRCA2genes can be carried out on a DNA sample from an affected family member. At present, centres able to offer mutation analysis select only those families most likely to have the currently identified genes (BRCA1 and BRCA2) since the analysis is very time consuming and expensive. In addition, a negative result does not substantially alter breast cancer risks in most circumstances as most techniques will be unable to identify 20-30% of disease causing mutations and other, as yet unidentified, genes may give rise to less striking family histories. There is good evidence that isolated early onset breast cancer cases or clusters of two or three later onset breast cancer cases are unlikely to be the result of a mutation in one of these genes.20-22 However, families with four or more breast or ovarian cancer cases are much more likely to be the result of BRCA1 orBRCA2 mutations.22
It is in only a small proportion of those families in whom mutation analysis is possible that a mutation is found and, therefore, a test can be offered to other family members. If a mutation is detected which is clearly causing the cancer prediposition, predictive (presymptomatic) testing can be offered to any family member by the genetics service. Presymptomatic testing involves, in most cases, a session to disclose all the relevant information, explore the subject's expectations and concerns, and then a further session with a minimum of four weeks “cooling off” period before the test sample being taken. The result is given (disclosure) usually face to face and further follow up is arranged thereafter according to the result and the needs of the person. Current experience is that the numbers of men and women proceeding with predictive testing is much smaller than those who express an interest.
Since a disease causing mutation is detected in only a minority of families examined, and in the UK the mutation analysis of bothBRCA1 and BRCA2may take several months at best, starting to search for aBRCA1 or BRCA2mutation in a family may well not alter the clinical decisions facing that family for a considerable time, if at all. Where a mutation has been found in an affected family member and predictive testing is possible, a negative result allows disinvestment in breast and ovarian screening or surgery. A positive test result allows targeted screening and information on which to base choices about preventive measures, such as prophylactic mastectomy and oophorectomy or chemoprevention. Furthermore, management of breast cancer, if diagnosed, may differ for women with a known genetic predisposition. For example, for an oestrogen receptor positive tumour where there is thought to be a significant future risk of ovarian cancer (for example,BRCA1 or BRCA2), surgical removal of the ovaries as an adjuvant treatment may be a better choice than either a radiation induced menopause or other hormonal manipulation, particularly if this is shown to reduce the risk of recurrence or new primaries in this situation. In addition, the risk to the contralateral breast approaches 40-50% at 10 years23 and must be discussed. Predictive testing should be carried out only within the framework of the Regional Clinical Genetics Service using accredited molecular genetics laboratories. Adequate follow up is needed for subjects undergoing predictive testing and in some cases psychological support may be needed.
Summary
Guidelines should ideally be based on evidence if they are to be implemented.24 For the present, evidence of a benefit of mammographic screening aged 40 to 49 years is emerging,25-27 but evidence on the outcome of breast screening in women under 40 years of age is very limited. Preliminary evidence from a reanalysis of the Swedish Two Country Study25 26 and from a recent meta-analysis27indicates a slight survival advantage for screening women aged 40 to 49 years. Data from large breast cancer family history clinics28 29 suggest that regular mammography can successfully detect early stage cancer in women under 50 years of age with an increased risk owing to family history. The data from both the general and the high risk population have suggested that screening on a 12 to 18 monthly basis will be necessary as the mean sojourn time (lead time) is 1.25 to 1.5 years in the under 50 age group.30Table 1 presents the current consensus view of the UK Cancer Family Study Group of what type of family history is likely to indicate low, moderate, or high risk of breast cancer based on family history. It is worth remembering that epidemiological factors such as late age at first birth can statistically increase risk of breast cancer as much as 2-3 fold and this is not currently viewed as a reason for introducing additional or early mammography. Genetic risks fall with increasing age so women who might be eligible at 40 for additional mammography on grounds of genetic risk might fall back into a lower risk group once they enter the NHS BSP at 50 years. Very few women will ultimately be able to undergo predictive genetic testing; many more will be eligible for trials of screening, chemoprevention, and even dietary intervention. Most of the women who enter into a screening programme will not develop breast cancer. Although cancers can be detected early with conventional screening methods, a clear cut benefit in terms of mortality reduction from any of the interventions available has yet to be proven and large scale prospective clinical trials are urgently needed. Quality assurance for such screening trials should be as rigorous as for the established breast screening programme.
The guidelines set out in this paper and similar guidelines, such as those produced recently by the British Association of Surgical Oncology Specialist Breast Group31 should be viewed as a framework for the UK and could form the basis of large scale collaborative studies aimed at gathering evidence to produce definitive guidelines for planning health care in the future.
References
Footnotes
-
* UKCFSG Steering Committee: Professor DT Bishop (Secretary), Professor J Burn (Chairman), Mrs P Chapman, Professor E R Maher, Dr D Easton, Dr D Eccles, Dr R Eeles, Dr P Hopwood, Dr R Houlston, Dr S V Hodgson (ICRF), Dr F Macdonald, Dr J Mackay, Professor B A J Ponder (CRC)