Article Text

Abstract
Introduction: Studies on the role of the insertion/deletion (I/D) polymorphism of the gene coding for angiotensin converting enzyme (ACE) in atherosclerosis have been inconsistent. In a meta-analysis, we recently showed that this relationship is stronger in high risk populations. In this paper, we used a combined functional and population based approach to investigate the gene–environment interaction of the ACE I/D polymorphism in relation to carotid artery wall thickness.
Methods: The study was part of the Rotterdam Study, a prospective population based cohort study. In 5321 subjects, IMT was measured in the carotid arteries by ultrasonography and ACE genotype was determined by size analysis of polymerase chain reaction products.
Results: In multiple regression analysis, I/D polymorphism and smoking were the main determinants for plasma ACE activity (r2 = 0.28). There was a positive association between the D allele of the I/D polymorphism and carotid artery thickness among current smokers (p = 0.03). Subjects carrying only one of the risk factors (smoking or the D allele) did not show significant differences in IMT compared with the non-/former smokers group carrying two II alleles, while carriers of both risk factors had significant higher IMT. The association was not present in non-/former smokers.
Discussion: The results provide further evidence that genetic and environmental factors interact in the formation of the arterial lesions. This study shows that large population based studies can be extremely helpful in unravelling the genetic origin of complex diseases such as atherosclerosis.
- angiotensin
- atherosclerosis
- genes
- smoking
- ACE, angiotensin converting enzyme
- I/D, insertion/deletion
- IMT, intima media thickness
- NO, nitric oxide
Statistics from Altmetric.com
- ACE, angiotensin converting enzyme
- I/D, insertion/deletion
- IMT, intima media thickness
- NO, nitric oxide
Angiotensin converting enzyme (ACE) is a key component in the renin angiotensin system, converting angiotensin I to angiotensin II.1 It also inactivates vasodilator bradykinin. Both peptides play central roles in blood pressure regulation and are believed to be important in the pathogenesis of cardiovascular diseases. ACE levels in plasma and tissue are under genetic control.2–4 There is a common insertion/deletion (I/D) polymorphism in the ACE gene characterised by the presence or absence of a 287 bp alu repeat. Subjects with the DD genotype have higher plasma ACE activity compared with those with ID and II genotypes.2,3 This finding predicts that carriers of this genotype may have increased blood pressure and a higher prevalence of cardiovascular diseases.
Findings on the association between the ACE I/D polymorphism and atherosclerosis using ultrasonographic measurements of carotid arteries have been inconsistent. Some studies showed a relation of atherosclerosis with presence of the D allele,5–8 while others have failed to show such association.9,10 The majority of the studies conducted until now were based on relatively small sample sizes, which may in part explain the inconsistency, particularly when interactions were studied.11 A recent evaluation of candidate gene studies in a meta-analysis demonstrated that large studies are needed to show the effects of the genes involved in complex traits.11 Recently, we performed a meta-analysis of the association between this polymorphism and carotid artery intima media thickness (IMT), using all studies conducted until October 2002.12 When pooling the data of 23 articles (9833 subjects), we found that carriers of the DD genotype have an increased thickness of common carotid IMT. The correlation was most pronounced in high risk populations, suggesting gene–environment interactions.12
From our meta-analysis, it is not clear which factor is interacting with the ACE gene. As studies of gene–environment interactions are prone to false positive and negative findings, we used a combined functional and population based approach. To unravel the role of interactions of the ACE I/D polymorphism with other factors, we aimed to identify the non-genetic determinants of the renin angiotensin system, specifically those associated with serum ACE activity. We studied various vascular risk factors in relation to ACE activity and found that only smoking was a determinant of ACE activity in addition to the ACE gene. As a second step, we investigated ACE and its interaction with smoking in relation to carotid ultrasonographic measurements and found evidence that smoking is a factor modifying the prevalence of ACE related carotid artery lesions.
METHODS
Study population
This study is part of the Rotterdam Study, an ongoing population based follow up study designed to investigate the determinants of chronic diseases in the elderly; it has been described in more detail elsewhere.13 In brief, baseline data were collected between March 1990 and July 1993 from 7983 subjects, aged 55 years or older, living in Rotterdam, the Netherlands.13 The study was approved by the medical ethics committee of Erasmus University, and written informed consent was obtained from all participants.
All participants were interviewed at home by a trained research assistant using computerised questionnaires, and they subsequently visited the study centre. Smoking history was assessed during the interview at home and patients were categorised as never, former, or current smokers. At the study centre, an extensive physical examination was performed on each patient, including ultrasonography of the carotid arteries. A blood sample was drawn, and serum and plasma were stored at −80°C.
Carotid ultrasonography
Carotid atherosclerosis was assessed by duplex scan ultrasonography of the carotid arteries, using a 7.5 MHz linear array transducer (ATL, Ultramark IV). Measurements of IMT were performed offline from the still images recorded on videotape. Details about this measurement have been published previously.14 Briefly, the interfaces of the far and near walls of the distal common carotid artery are marked over a length of 10 mm. We used the average of the measurements of three still images of both the left and right arteries. Carotid IMT was determined as the mean of the maximum IMT of near and far wall measurements of both the left and right arteries. Results from a reproducibility study of IMT measurements have been published elsewhere.15 The mean (SD) differences in common carotid IMT between paired measurements of sonographers, readers, and visits were 0.005 (0.09) mm, 0.060 (0.05) mm and 0.033 (0.12) mm, respectively.
We defined plaques as focal widening of the vessel wall with protrusion into the lumen, composed of calcified or non-calcified components. The protrusion was evaluated by eye, without measuring the thickness of the lesions or of the adjacent structure. The total plaque score reflected the total number of sites with plaques and ranged from 0 to 6 (left and right sided common carotid arteries, bifurcation, and internal carotid arteries).
Laboratory assessments
Colorimetric determination of ACE activity was performed in the stored plasma samples (−80°C). Because of cost considerations, ACE levels were assessed in a random group of 215 individuals. The measurements were carried out with a kit by Fujirebio Inc, which uses a p-hydroxy-Hip-His-Leu substrate.16 Fluorimetric assay of ACE activity in plasma was performed by measuring the release of His-Leu from the substrates Hip-His-Leu and Z-Phe-His-Leu.17,18
DNA was isolated from the blood samples using standard procedures (salting out).19 The II, ID, and DD genotypes were detected by PCR according to the method of Lindpaintner et al20 with some modifications. The insertion and deletion alleles of the ACE gene were identified by using a set of oligonucleotide primers flanking the polymorphic site in intron 16. The final volume of the PCR mix was 20 μl, containing 50 ng DNA as template and 1×PCR buffer (Gibco), 1.3 mmol/l MgCl2, 200 μmol/l dNTPs, 20 pmol primer mix and 0.35 U Taq polymerase in a PE9600 PCR machine. The thermocycling procedure was completely identical to the method of Lindpaintner et al.20 The result of amplification was a 319 bp and a 597 bp amplicon for the D and I alleles respectively.
Because the D allele in heterozygous samples is preferentially amplified, there is a tendency towards misclassification of about 4–5% of ID genotypes to DD. In order to avoid this, a second independent PCR was performed with a primer pair that recognises an insertion specific sequence. To optimise the second PCR, 10% DMSO, 0.35 U AmpliTaq Gold DNA polymerase and 1× GeneAmp PCR Gold buffer (Applied Biosystems) was added to the PCR mix with annealing temperature of 67 °C. The reaction yielded a 335 bp amplicon only if the I allele was present. All reactions were performed in 96 well plates and handled by a robot (Beckman Biomek® 2000).
In the post-PCR analyses, 10 μl of PCR product was loaded onto a 3% agarose gel. Fragments were visualised using etidium brominde staining and UV transillumination. Two independent investigators interpreted the pictures from each gel and all ambiguous samples were analysed a second time.
Statistical analyses
Hardy-Weinberg equilibrium was tested with the χ2 test. We analysed the distribution of conventional cardiovascular risk factors among three genotype groups by χ2 analyses for dichotomous variables and by one way analysis of variance for continuous variables. Multiple linear regression analysis was used to analyse the relation between vascular risk factors and ACE activity. The differences in ACE activity and IMT between the smoking and genotype groups were tested using the general linear model univariate procedure, adjusted for age and gender. In addition, subjects were divided into two groups based on the number of plaques in the carotid arteries (0–2 and ⩾3 plaques). Logistic regression was used to estimate the adjusted odds ratios for the different genotype groups using subjects with the II genotype as reference. No adjustments were initially made for vascular risk factors such as hypertension, as they may act as intermediate factors. Interaction of the ACE genotype with smoking was tested using a multiplicative model. All statistical analyses were conducted using SPSS for Windows (version 11.0).
RESULTS
We performed our analysis on 5321 subjects for whom the complete data for ACE genotyping, IMT measurements, and smoking status were available. Data for at least one of the variables were missing in the remaining subjects due to logistic reasons; mainly because the subjects were too old or disabled to visit the research centre for the examination. In our sample, the frequency of the D allele was 53.3% and the distribution of the genotypes and allele frequencies were in Hardy-Weinberg equilibrium (II, 21.7%; ID, 49.9%; and DD, 28.3%; p = 0.82). Among the remaining subjects for whom the genotype frequencies were available (n = 1548), no deviation from Hardy-Weinberg equilibrium was observed. Furthermore, there was no significant difference in the genotype frequencies between the two samples (p = 0.44).
Table 1 shows the demographic characteristics of the participants by ACE genotype. No significant differences were found among the three genotypes with respect to classical cardiovascular risk factors. The carriers of the D allele were significantly older than the II carriers but the difference was only 1.22 years. Furthermore, carriers of the DD genotype had a significantly higher mean systolic blood pressure and a higher mean of carotid IMT compared with the II genotype. Although there was a slight increase in the percentage of subjects with three or more plaques, the frequency did not increase significantly in carriers of the D allele compared with the II genotype (table 1).
Demographic characteristics of subjects according to ACE I/D genotype
In the sample of 212 individuals for whom both plasma ACE activity and I/D genotypes were measured, the allele and genotype proportions were consistent with Hardy-Weinberg equilibrium (p = 0.48). In multiple linear regression analysis, ACE I/D polymorphism and smoking were the only determinants of plasma ACE activity (table 2). These two factors together explained 28% of the variation in enzyme levels in serum (r = 0.53, p<0.01). The activity of ACE was not significantly different between former and non-smokers (14.83 (3.57) and 15.58 (3.87) U/L respectively), therefore we combined these two groups. Overall, the ACE activity was 1.8 U/L higher in current smokers compared with non-/former smokers (p<0.01). Although the difference in ACE activity between smokers and non-/former smokers was largest in the ID and DD group, it was not significantly different from the difference in the II group (fig 1).
Vascular risk factors and their association with plasma ACE levels

Plasma ACE activity in different genotypes stratified by smoking status. Data are adjusted for age and gender. *Significantly different from the genotype II non-/former smokers group.
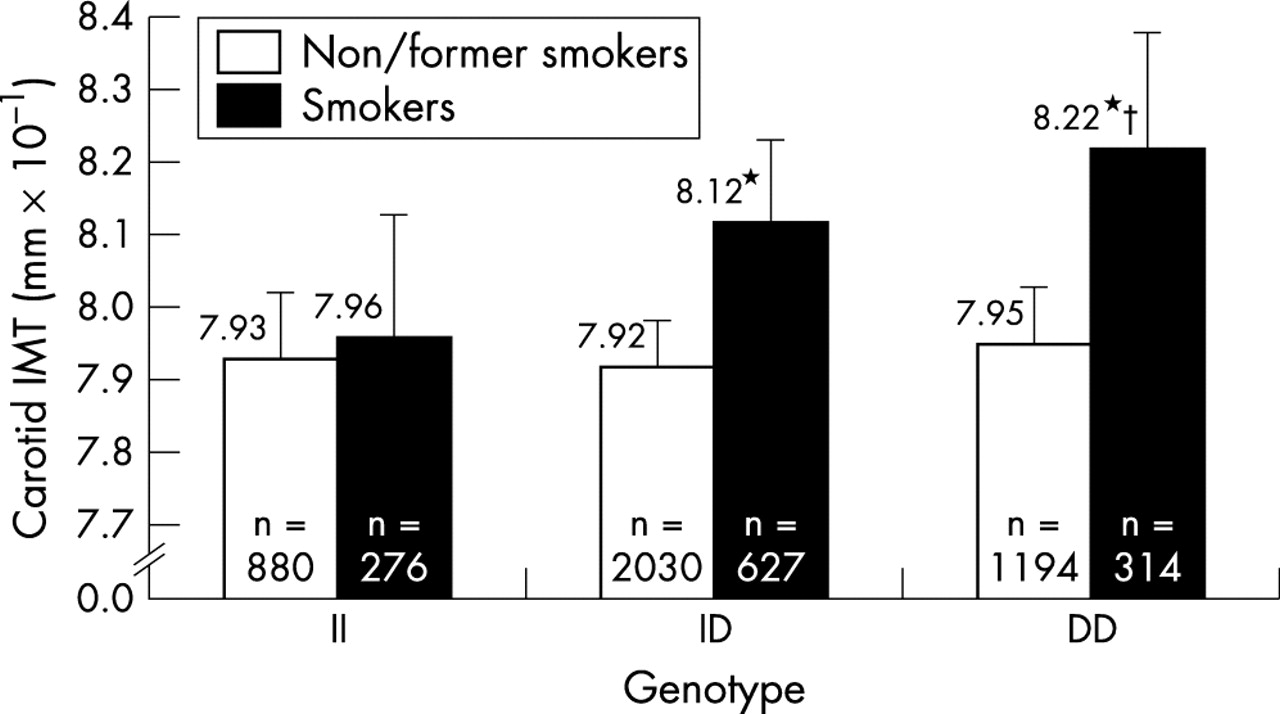
When studying the joint effect of smoking and the ACE gene on IMT, there was a significant increase in mean carotid IMT in those carrying the D allele in current smokers (p value for trend was 0.04). The IMT difference (mean (SE)) between DD and II genotypes in smokers was 0.26 (0.12) mm×10−1 (p = 0.03). In contrast, IMT was not significantly associated with the D allele among non-/former smokers (fig 2). The p value for interaction between ACE genotypes and smoking status was 0.08. The differences between genotype groups in smokers reduced but did not disappear when adjusted for systolic blood pressure. Subjects carrying only one of the risk factors (smoking or the D allele) did not show significant differences in IMT compared with the genotype II non-/former smokers group, while carriers of both risk factors had significantly higher IMT (p<0.01).
{kind=link}
{kind=link}
Carotid intima media thickness (IMT) level in different genotypes stratified by smoking status. Data are adjusted for age and gender. *Significantly different from the genotype II non-/former smokers group. †Significantly different from the genotype II smokers group.
The odds ratios of having three or more plaques in carotid arteries in current smokers were 1.14 (95% confidence interval (CI) 0.81 to 1.59) and 1.40 (95% CI 0.96 to 2.04) for ID and DD genotypes respectively. This increase of odds ratios with the number of the D alleles was borderline significant (p = 0.07) while in non-/former smokers the odds ratios remained the same between genotype groups.
Stratified analyses concerning the combined effect of ACE polymorphism and other cardiovascular risk factors (hypertension, hyperlipidaemia, diabetes, obesity, age, and gender) on carotid IMT did not show any significant difference among and between the stratified groups. In all the analyses, the mean IMT difference between DD and II genotypes was less than 0.20 mm×10−1 and did not reach significance level (p>0.10).
DISCUSSION
In this study, we found a modest but significant association between the ACE I/D polymorphism and carotid IMT in the presence of smoking. In non-/former smokers, no significant association between the ACE genotype and IMT was observed.
This study is the largest population based study performed on ACE I/D polymorphisms and carotid artery lesions. The next largest study, which used a sample size of 3657 individuals in Japan,21 failed to find a relation between ACE and IMT. Difference in ethnicity could be a possible explanation; however, the problem in comparing findings is that the interaction between ACE polymorphism and smoking was not studied by Mannami et al.21 Findings of other studies on the interaction between the ACE gene and smoking have not been consistent. An interaction between smoking and ACE I/D genotype on atherosclerosis was reported in 1997 by Hibi et al,22 who showed a smoking associated effect of the ACE genotype on the severity of coronary atherosclerosis.22 Another study23 found an association between ACE I/D and carotid IMT only among non-/former smokers, particularly those on chronic cardiovascular medication. Yet others failed to find evidence for such an interaction.24
Genetic studies aiming to uncover gene interactions are extremely prone to false positive and negative findings. To obtain internal consistency in our study, we studied not only the relation of the ACE gene to atherosclerosis but also to ACE activity, which have been studied extensively with regard to polymorphisms in the ACE gene.25–28 Since Rigat et al2 reported in 1990 that the ACE I/D polymorphism determines the plasma activity of the enzyme, many studies have replicated this finding.3,8,10 Our data also confirm that the presence of the deletion allele is significantly associated with the plasma ACE activity. The ACE activity values in our study were in the same range as those from other population studies, which used the same method of measurement.8,29 Although ACE levels were determined in stored sera and laboratory drift may have occurred, such drift is unlikely to be associated with the ACE genotype.
To unravel the role of interactions of the ACE I/D polymorphism with other vascular risk factors, we focused on identifying the determinants in the renin angiotensin system, specifically those associated with serum ACE activity. In our population based study, we found that smoking is the only other factor related to plasma ACE activity, suggesting that they use the same pathways. The vascular risk factors that might be related to serum ACE activity are not well known. In one report, smoking and blood pressure30, and in another, male sex and history of hypertension31correlated with the serum ACE activity. In our sample, the I/D polymorphism and smoking together explained 28% of the variance in ACE activity. On average, current smokers had 1.8 U/L higher ACE activity in plasma. Although the differences were not significant, in those carrying the ID and DD genotypes the effect of smoking on ACE activity was larger than in the II genotype. A possible effect of smoking on cleavage secretion of ACE from the endothelial cells may explain this finding.32 Additionally, there are indications that nicotine increases expression of a number of genes in the endothelium, including ACE.33
The values for IMT in our study strongly concurred with those reported by Tabara et al, using a sample with the same age.34 In order to test if the observed association between the I/D polymorphism and carotid IMT in the presence of smoking was through blood pressure, we adjusted our analysis for systolic blood pressure. Our result suggests that blood pressure does not fully explain the association. Recently, it has been shown that the DD genotype is associated with a significant blunting in vasodilatation through nitric oxide (NO) pathways (due to increased angiotensin II induced NO breakdown and/or reduced bradykinin mediated NO release).35 This finding is followed by other studies showing that smoking decreases plasma NO level36 that may lead to impaired endothelium dependent vasodilation.37,38 In addition, NO has important anti-oxidative capacities, and smoking induces oxidative stress by reducing concentrations of NO and other antioxidants in plasma.39 Concurrently, carriers of the DD genotype show a lower antioxidant response compared with II and ID genotypes.40 The above observations suggest that carriers of the DD genotype who smoke are likely to be at higher risk of atherosclerosis.
Using a combined functional and population based approach provides us with an a priori hypothesis for the environmental factor(s) that may interact with the gene. However, the question remains if other environmental factors can show the same pattern of interaction. The results of the stratified analyses showed no significant evidence for joint effect of the ACE polymorphism and other factors, prompting smoking as the best candidate for this interaction.
In summary, we found a positive association between the D allele of the I/D polymorphism and carotid IMT in the presence of smoking. This association provides further evidence that genetic and environmental factors interact in the formation of the arterial lesions. There may be various pathways underlying the observation of an effect of the ACE gene on IMT in smokers only, but on the basis of the present results it is not possible to fully explain the underlying mechanism. Our findings remain to be confirmed in future studies.
Acknowledgments
This study was supported by the Netherlands Organization for Scientific Research (NWO), grant 904-61-196.