Article Text

Abstract
Background and aims: Germline mutations in the CDH-1/E-cadherin gene are, to date, the only known cause of hereditary diffuse gastric cancer (HDGC). While two recent series of prophylactic gastrectomy described microscopic foci of signet ring cell carcinoma in sample sections from 10 macroscopically normal stomachs, whole stomach phenotype has not been mapped. We aimed to describe the size and distribution of foci in relation to mucosal zones and anatomical location.
Methods: Six patients (from three HDGC kindred) were referred for total gastrectomy via three different referral pathways. Following fixation, five stomachs were completely blocked and one extensively sampled. Histopathology was mapped to a mucosal photograph of each stomach, enabling precise localisation of carcinoma foci, benign pathology, and mucosal zones.
Results: There were 4–318 microscopic foci of intramucosal signet ring cell adenocarcinoma in the six macroscopically normal stomachs (foci size 0.1–10 mm in diameter). The distal third of the stomach contained 48% of total foci (range 29–75%). The body-antral transitional zone occupied 7.7% of mucosal area (range 3.6–11.8) but had 37% of foci (range 10%–75%). The largest foci were found in the transitional zone and foci density was five times greater in the transitional zone than in body or antral type mucosa.
Conclusions: In germline CDH-1 mutation carriers, multiple microscopic foci of intramucosal signet ring cell carcinoma show a predilection for the distal stomach and the body-antral transitional zone. Targeting the transitional zone would maximise the likelihood of finding foci in macroscopically normal gastrectomies, and particular attention should be paid to this area during endoscopy.
- hereditary diffuse gastric cancer
- E-cadherin
- signet ring cell carcinoma
- transitional zone
- gastrectomy
- genetic susceptibility
- HDGC, hereditary diffuse gastric cancer
- H&E, haematoxylin and eosin
- EGC, early gastric cancer
Statistics from Altmetric.com
- hereditary diffuse gastric cancer
- E-cadherin
- signet ring cell carcinoma
- transitional zone
- gastrectomy
- genetic susceptibility
The first indication of the identity of a major gastric cancer susceptibility gene was a genetic linkage analysis in a large New Zealand family of Maori ethnicity with diffuse gastric cancer.1 The predisposing gene mapped to an interval on chromosome 16q22.1 containing the gene for the cell to cell adhesion protein E-cadherin (CDH-1). Subsequent mutation analysis identified inactivating germline CDH-1 mutations in this family and two other Maori families with familial diffuse gastric cancer.1 E-cadherin is a member of the cadherin family of homophilic cell adhesion proteins that are central to the processes of development, cell differentiation, and maintenance of epithelial architecture.2 It is the predominant cadherin family member expressed in epithelial tissue and is localised at the adherens junctions on the basolateral surface of the cell. E-cadherin is downregulated in a broad range of epithelial tumours and its loss is associated with an infiltrating phenotype and poor prognosis.3–6
In 1999, incorporating data from other diffuse type gastric cancer kindred of different ethnicities with a confirmed CDH-1 germline mutation, a new dominantly inherited familial cancer syndrome was defined and named hereditary diffuse gastric cancer (HDGC).7 One mutated copy of the gene is inherited and somatic inactivation of the second CDH-1 allele results in reduced or absent E-cadherin expression.8 A study of the incidence of advanced gastric cancer in 11 different HDGC kindred (476 individuals) showed that gene penetrance is incomplete. The cumulative risk of advanced gastric carcinoma by 80 years of age was 69% in men and 83% in women.9 The combined mean age at diagnosis across the 11 kindred was 40 years (range 14–85) however this varied from 28 years in one Maori kindred to 62 years in another kindred from the USA. The reasons for this variation remain unknown; possibilities include genetic heterogeneity between different CDH-1 mutations, other gene-gene interactions, or environmental factors.9
Recently, the first two series of prophylactic gastrectomy in North American HDGC families were reported, with five cases in each.10,11 All 10 cases (mean age 36 years) showed microscopic foci of intramucosal signet ring cell carcinoma in macroscopically normal stomachs. To further characterise the early phenotype of this new cancer syndrome, our aim was to look for a pattern in the distribution and size of foci in relation to mucosal zones, proximal versus distal stomach, and benign pathology. To do this, the whole stomach was examined microscopically, and the precise location of benign pathology, mucosal zones, and cancer foci were mapped in gastrectomy specimens from three different HDGC families.
PATIENTS AND METHODS
Patients
Six total gastrectomy specimens from members of three different Maori HDGC kindred were studied (table 1). There were three pathways to surgical referral. Patients A (40 year old male), B (28 year old male), C (15 year old female), and D (34 year old female) are members of the kindred in whom CDH-1 germline mutations (a 1008-G→T truncating mutation) were first described (family A).1 They were referred from a chromoendoscopic surveillance programme that used methylene blue and congo red.12 Standard white light endoscopy was normal in each case. Biopsy of pale areas visible after congo red staining showed signet ring cell carcinoma. Assessment of Helicobacter pylori status involved biopsy and serology. Patient D had H pylori gastritis diagnosed on endoscopic biopsy one year prior to starting chromoendoscopy, and had been treated with triple therapy. Patients A, B, and C had no evidence of previous infection with H pylori.
Patient characteristics, CDH-1 mutation, and endoscopy details
Patient E (43 year old female) is from a kindred with a 1792-C→T truncating mutation. She elected to have a prophylactic gastrectomy. Fourteen months prior to surgery, endoscopic biopsy had demonstrated H pylori gastritis which was treated with triple therapy. The stomach had a normal appearance on repeat standard endoscopy six months later (eight months prior to gastrectomy). The eight biopsies taken (antrum lesser curve×2, mid-body greater curve ×2, upper body greater curve×2, and cardia×2) all showed mild chronic gastritis. No H pylori organisms were seen and the urease test was negative.
Patient F (33 year old female) is from a kindred with a 2287-G→T truncating mutation. Standard endoscopy demonstrated mild antral erythema. Biopsy of an antral ulcer (4 mm) in the early healing stage showed signet ring cell carcinoma. The remainder of the stomach was normal, as were two biopsies from the body mucosa. She did not have H pylori on biopsy or urease test. She was treated with proton pump inhibitors. Endoscopy was repeated 13 days later to try to determine the extent of carcinoma but the stomach was macroscopically normal with no sign of the previous ulcer. Twenty one random biopsies were taken from all areas of the stomach and all showed normal mucosa apart from a few scattered chronic inflammatory cells.
Method
Specimen processing
Fresh gastrectomy specimens were opened along the greater curve and pinned onto corkboard. The mucosa was carefully inspected before fixation in 10% formalin. Omental fat was dissected off and lymph nodes retrieved. Fixed stomachs from patients A–E were placed between two sheets of overhead projector transparency and the mucosal side photocopied. This mucosal photocopy was used as a life sized template to identify the exact location of tissue blocks. Stomachs were cut into 3 mm slices, with 1–3 slices of stomach wall per block. Coloured inks were used for orientation. Gastrectomy from patient F was processed in a different centre using a hand drawn map as template. The slides and map were reviewed (by AC). Patients B–F had their whole stomach blocked: a total of 247, 183, 207, 271, and 139 blocks, respectively. Patient A had extensive sampling from all areas of the mucosa (a total of 72 blocks) comprising approximately 30% of the mucosal surface area.
Mapping of foci of carcinoma, mucosal zones, and stomach thirds
A standard histological technique was used—that is, a single 4 μm haematoxylin and eosin (H&E) section from each 3 mm slice of paraffin embedded tissue was evaluated. Sections were screened at 100× (10×objective×10×ocular). Foci of carcinoma consisted of signet ring cells in a diffuse pattern, deep to the basement membrane, in the lamina propria. Foci of carcinoma larger than 3 mm in diameter (the width of a slice of stomach tissue in a paraffin block) occurring at the same position in contiguous slices were considered to be the same focus of carcinoma. Foci of carcinoma smaller than 3 mm (the majority) were counted as separate foci of carcinoma.
Mucosa type was categorised as oesophageal, body/fundic, body-antral transitional zone, antral, or duodenal type. The proximal border of the body-antral transitional zone was defined by gastric pit depth being quarter or less of mucosal thickness and relative paucity of deep mucous glands. The reliability of this method was confirmed by the absence of G cells using gastrin immunohistochemistry stains in sample sections (seven from patient A, two from patients B, C, D, and E).13,14 The distal border of the transitional zone was defined by the absence of chief cells.15 Mucosa type, location of foci of carcinoma, intestinal metaplasia, atrophy, and other non-neoplastic findings were mapped to respective mucosal photographic templates. The area of each mucosal zone was determined using ImageJ software (public domain) to trace zone perimeters on the digital images. Respective mucosal zone areas are expressed as a percentage of total mucosal area for each stomach. A foci density index (% foci/% area) was calculated and p values determined using the χ2 test.
The junctions between the upper, middle, and lower thirds of the stomachs were determined using the method described by the Japanese Research Society for Gastric Cancer: the three portions are delimited by dividing the lesser and greater curvatures at two equidistant points and joining these points.16 The number of foci were counted in each stomach third and in the three mucosal zones.
RESULTS
All six macroscopically normal gastrectomies had multiple microscopic foci of diffuse signet ring cell carcinoma, with negative lymph nodes (table 1). All foci were intramucosal. The number of foci of carcinoma per stomach varied from four in patient E to 318 in patient C. The smallest focus was 0.1 mm in diameter, the largest 10 mm (fig 1A, B). Most foci were less than 1 mm in diameter. Foci were present on the apex of rugal folds and the area gastricae. Neither in situ signet ring cell carcinoma nor dysplasia was seen. No mitoses were seen in any of the foci of signet ring cell carcinoma.

(A) Patient B: 0.2 mm focus of intramucosal diffuse signet ring cell carcinoma. Signet ring cells infiltrate between normal gastric pits and under normal gastric surface epithelium, in the superficial lamina propria (original magnification 40×). Inset: central area showing typical signet ring cell morphology (original magnification 400×). (B) Patient A: part of 9 mm focus, occupying the left two thirds of the frame; normal mucosa on the right third. Signet ring cells occupy the full thickness of the mucosa under intact epithelium (original magnification 100×). Inset: signet ring cells in the lamina propria (original magnification 400×). Haematoxylin and eosin stained sections.
Patient A had 45 foci in the 30% of mucosa surface area blocked, including all of the antrum. This was the first gastrectomy performed in this series and complete mapping was not possible because the remaining tissue was destroyed. Foci were found in the body and transitional zone but not in the antrum (see table 2, fig 3). The largest focus was 9 mm in diameter. It was located in the body-antral transitional zone at the incisura.
Distribution of cancer foci by anatomical thirds and mucosal zones

Stomach maps showing location and size of carcinoma foci and mucosal zones. Gastric mucosal zones shown by translucent colours on gastrectomy photograph. Black circles are carcinoma foci, to scale, except foci <1 mm which are shown arbitrarily as 1 mm for visibility. F, defect caused by removal of fresh tissue for cryostorage. (A) Patient E: four foci, three in the body-antral transitional zone. (B) Patient B: 214 foci, greatest density in the body-antral transitional zone. (C) Patient C: 318 foci, greatest density in the body-antral transitional zone. (D) Patient D: 111 foci.
{kind=link}
{kind=link}
{kind=link}
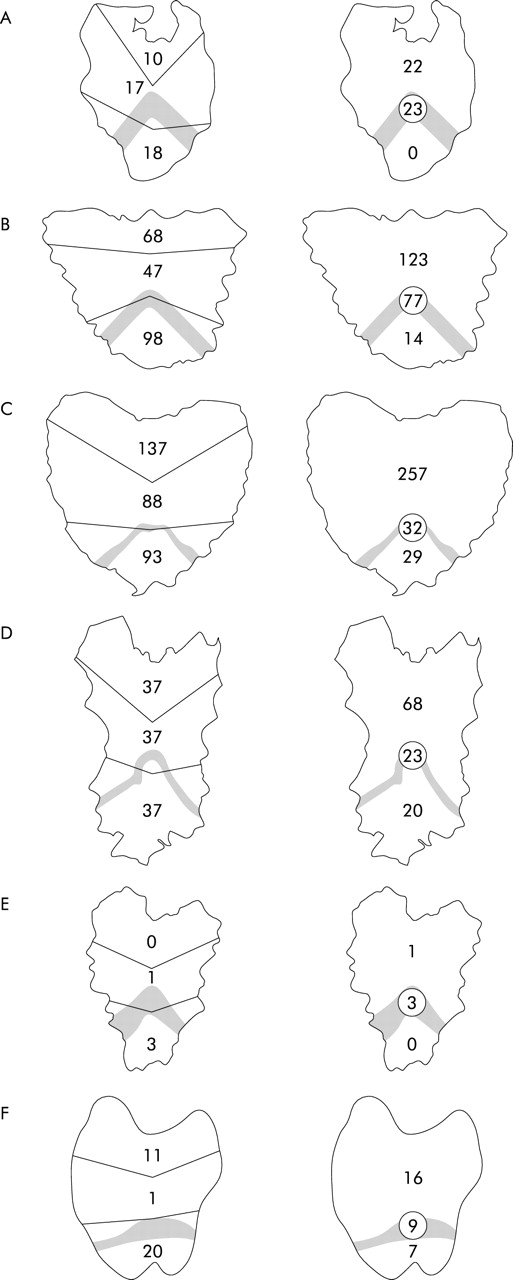
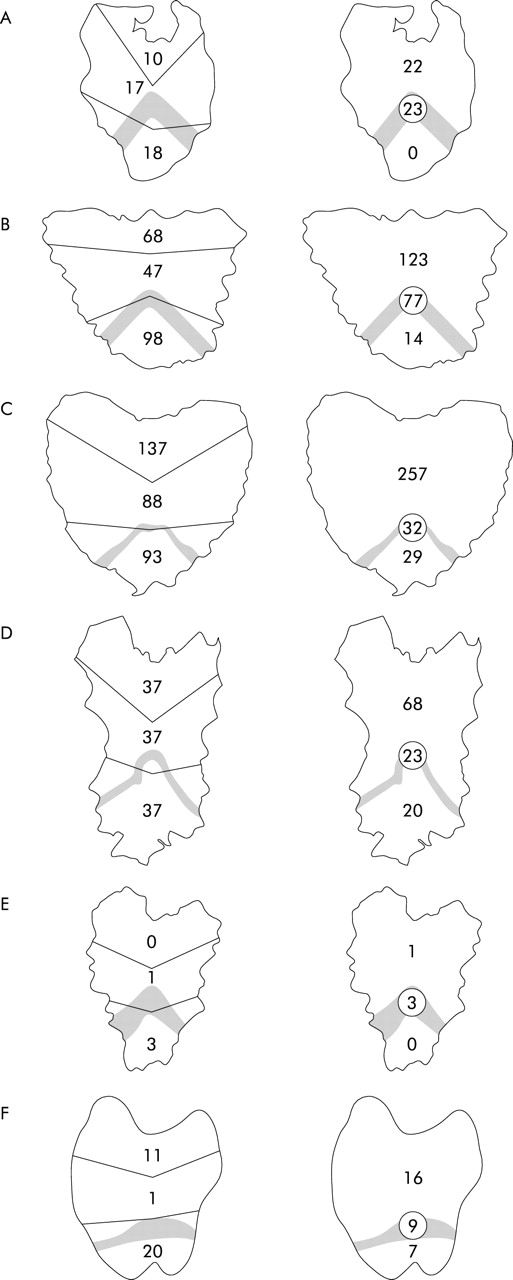
Distribution of carcinoma foci by anatomical location and mucosal zones in patients A–F. Left row: division by thirds; right row: division by mucosal zones. The body-antral transitional zone is shaded. Number of foci in the respective areas are indicated on the diagram.
Patients B–F had the whole stomach blocked (see table 2, fig 3). The greatest number of foci were found in patient B (214 foci; fig 2B) and patient C (318 foci; fig 2C). In these stomachs, the largest foci and greatest density of foci were in the transitional zone. Patient D had 111 foci (fig 2D) with the largest focus (4 mm) in the proximal antrum. In contrast, patient E (fig 2A) had only four foci but three of these were in the body-antral transitional zone. Patient F had 32 foci located in all zones, the largest focus was 4.5 mm, and it was in the body-antral transitional zone.
Looking at foci distribution with respect to gastric mucosal zones (fundic/body, body-antral transitional, and antral), the proportion of foci in each mucosal zone was calculated as a percentage of the total number of foci present in each stomach (tables 2, 3). Foci were found in the body-antral transitional zone in all six stomachs, including the largest foci in all, except patient D. The transitional zone occupied 7.7% of the total mucosal area (range 3.6–11.8%) but contained 37% of foci (range 10–75%). Based on these values (table 3), a foci density index was calculated (% foci/% area); this was significantly (p<0.01) greater in the transitional zone (4.65) compared with either the body (0.70) or antrum (0.82).
Area of mucosal zones (as percentage of total stomach area) and foci per mucosal area (as percentage of total foci)
Looking at foci distribution by dividing the stomachs anatomically into upper, middle, or lower thirds, the proportion of foci in each third was calculated as a percentage of the total number of foci present in each stomach (table 2). The distal third contained the greatest number of foci, with 48% of total foci (range 29%–75%). The upper and middle thirds contained 27% and 25% of total foci, respectively. The body-antral transitional zone was predominantly located in the distal third.
Focal intestinal metaplasia was present in the antrum of patients E and F (fig 2A). This was not in the location of the carcinoma foci. The two patients who had previous H pylori infection (patients D, E) had no organisms or gastritis detected in their gastrectomy specimens. In patient C, there was chronic gastritis in the body mucosa consisting of numerous lymphoid aggregates in the basal mucosa, but no active gastritis, no intestinal metaplasia, and no H pylori organisms.
DISCUSSION
The microscopic foci of early HDGC were first described in two series of five prophylactic gastrectomies from three North American HDGC kindred.10,11 All 10 cases had no evidence of carcinoma on preoperative endoscopy and biopsy, and at resection the stomachs were macroscopically normal. In our series of six gastrectomies, all stomachs were similarly macroscopically normal although only one case was a prophylactic gastrectomy. This is consistent with the preoperative findings using white light endoscopy in these six patients (four patients had carcinoma detected by chromoendoscopy, patient F’s ulcer had healed). Despite close examination of the regions corresponding to the location of the respective endoscopic biopsies that had shown carcinoma, macroscopic abnormalities could not be detected.
The average age of patients in our series was 32 years, four years younger than the average age of the 10 patients who underwent prophylactic gastrectomy in the literature. Chun et al reported a series of five gastrectomies in members from one family; two patients had single foci (1 mm and 4 mm), one patient two foci (2 mm and 3 mm), another patient had five foci (1–3 mm), and the fifth patient “several” foci.11 Huntsman et al report similar findings from two HDGC kindred.10 In their first family, one stomach had two foci while the other had foci in 65 of 140 tissue blocks. In the three patients from their second family, one had unifocal disease and two had “multifocal” disease.
All 16 gastrectomies to date contained microscopic intramucosal signet ring cell carcinoma. The universal finding of carcinoma foci in this group of relatively young CDH-1 mutation carriers is interesting in the context of the 20–30% of CDH-1 mutation carriers who do not develop clinically evident gastric cancer in their lifetime.9 The youngest patient to have prophylactic gastrectomy so far was a 22 year old who had multifocal intramucosal carcinoma10 and, in our series, the youngest patient was a 15 year old who had 318 foci of intramucosal carcinoma.
There was wide variation in the number of foci per gastrectomy in our series, ranging from a stomach with only four foci to one with 318 foci. All foci were at the same stage. As most foci of carcinoma were less than 1 mm in size, the total number of foci counted per stomach is highly likely to be less than the true number of foci. This is because most of the tissue from each 3 mm slice remains in the paraffin block, unexamined. This is true of most histology. Factors that have induced multifocal disease in these CDH-1 germline mutation carriers are unknown although downregulation or inactivation of the remaining CDH-1 allele is likely to be a consistent genetic event in all foci. Hypermethylation of the CDH-1 promoter is common in both sporadic and inherited diffuse gastric cancer and could conceivably lead to the observed field effect.8,17 Furthermore, it is possible that variations in the density of CpG dinucleotide methylation within the CDH-1 promoter, which tends to be heterogenous in HDGC gastric tumours,8 is a determinant of the number of foci. It remains to be determined if specific genotype, physiological states, or environmental triggers can influence CDH-1 promoter methylation.
All signet ring cell carcinoma foci from the six gastrectomies involved the superficial lamina propria, lying beneath normal surface epithelium and between normal gastric pits. The finding of small early signet ring cell carcinoma beneath preserved surface epithelium has been described in sporadic gastric cancer.18 It has been suggested that this feature, the lack of desmoplastic stromal response, and the presence of intracytoplasmic mucin of predominantly neutral mucopolysaccharide all suggest a close histiogenetic relationship between signet ring carcinoma cells and the mucous neck cell in the basal region of gastric pits.18 Interestingly, in situ signet ring cell carcinoma was described in two prophylactic gastrectomies from the same HDGC family.10 We did not see any in situ carcinoma in the six gastrectomies from our series.
The diffuse phenotype in gastric cancer (hereditary and sporadic) is related to reduced E-cadherin expression.19 It has been suggested that loss of E-cadherin is the fundamental defect in diffuse type gastric carcinoma, and provides an explanation for the observed morphological phenotype: discohesive cells with loss of polarity and gland architecture.20 In contrast, gland architecture is preserved in the intestinal type of stomach cancer where loss of E-cadherin expression is not a feature.19
It is remarkable that in gastrectomies with 111, 214, and 317 foci, all were confined to the mucosa, and that all 16 cases reported mucosal disease only. This suggests that an indolent stage exists and further genetic events are required to allow mucosal escape. Early gastric cancer (EGC) is by definition confined to the mucosa or submucosa, and is independent of nodal status. When EGC is confined to the mucosa or is node negative, the reported five year survival is now over 90% in almost all Western and Japanese series.21 However, in HDGC, long term survival post-gastrectomy (either prophylactic or for early gastric carcinoma) is at present unknown.22
The predilection of sporadic EGC for the distal stomach has been previously described in a large Japanese series of 2562 lesions in 2300 cases that showed that 11% were in the proximal third, 56% in the middle third, and 33% in the distal third.23 In our six cases, there were a total of 724 foci, which overall show a distal stomach predilection, with 27%, 25%, and 48% of foci in each respective third moving from the proximal to distal. Analysis of foci distribution by stomach thirds can potentially overstate findings in stomachs with few foci, as in patient E with only four foci. If patient E is excluded from the analysis, the distribution is proximal third 33%, middle third 24%, and distal third 42%.
The relationship of foci location to the body-antral transitional zone is striking in patients B and C who showed the greatest density and largest foci in the body-antral transitional zone. The gastric transitional zones have recently been described as neglected areas of gastric anatomy with respect to possible links between these zones, H pylori ecology, peptic ulceration, and gastric cancer.15 The body-antral transitional zone is usually located two fifths along the lesser curve, while on the greater curve it has a slightly more distal location but is symmetrical on the anterior and posterior walls of the stomach.14 It is considered a dynamic area, exemplified by proximal migration in chronic gastritis.15
The location of the body-antral transitional zone was determined histologically in this study with the distal border defined by the absence of chief cells, which is easily determined on H&E alone. The proximal border of the transitional zone was defined by the absence of gastrin secreting G cells.13 G cells were identified by gastrin immunohistochemistry on sample slides, and then corresponding cytoarchitectural features assessable on H&E were used by proxy. Using chromoendoscopy, it is possible to approximate the region of the transitional zone. Congo red is a pH sensitive reactive vital dye (used in chromoendoscopy with intravenous pentagastrin to stimulate acid) and allows visualisation of the acid secreting stomach mucosa, reflecting parietal cell distribution.24,25
In this small series, the transitional zone occupied on average 7.7% of the mucosa surface area which is slightly higher than the 5% derived by Oi and colleagues26 in a study of 855 stomachs resected for peptic ulcer. The consistently higher proportion of total foci located within its boundaries (average of 37%) is notable. In addition, patients B and C, who had the greatest number of carcinoma foci, showed foci clustering in the transitional zone (fig 2B, 2C). Our method of calculation of mucosal area did not allow for extra surface area attributable to rugal folds, which are predominantly in the body area in our stomach maps. This would effectively result in underestimation of body mucosa surface area and consequent overestimation of relative transitional zone area.
There are a number of possible explanations for the predilection of carcinoma foci for the body-antral transitional zone: (i) epithelial cells in this region may be more vulnerable to genetic or epigenetic damage from luminal factors, for example because of reduced mucosal protection; (ii) the zone may be more conducive to the synthesis or action of carcinogens; (iii) variation in local acid output may produce an acid gradient across this zone affecting carcinogenesis.15 The theory that H pylori encounters its optimal pH for growth at some point along this gradient and provokes a more pronounced tissue response has been suggested in sporadic gastric cancer15; (iv) unique paracrine relationships that potentiate carcinogenesis may exist in the zone; (v) the zone may be more vulnerable to physical damage; and (vi) as all stomachs from this study were from Maori HDGC kindred, it is also possible, although unlikely, that environmental or genetic factors particular to Maori could affect the distribution and pathology of the carcinoma foci.
In summary, the multiple foci of intramucosal signet ring cell carcinoma in the stomachs from germline CDH-1 mutation carriers are predominantly located in the distal stomach, with the greatest density and largest foci in the body-antral transitional zone. If this distribution holds in further HDGC stomachs, then targeting the transitional zone would maximise the likelihood of finding microscopic foci. This has relevance in endoscopic surveillance and for pathologists dealing with macroscopically normal gastrectomies from these patients, and may also reveal clues to the pathogenesis of gastric cancer.
Acknowledgments
We thank Mr R Roberts, Department of Surgery, and Drs Lauree Hunter and Justine Gearry, Department of Pathology; Christchurch Hospital, New Zealand.
REFERENCES
Linked Articles
- Leading article
- PostScript
- Editor's quiz: GI snapshot
- Editor's quiz: GI snapshot
- Editor's quiz: GI snapshot