Article Text

Abstract
Background Variants in genes belonging to the tubulin superfamily account for a heterogeneous spectrum of brain malformations referred to as tubulinopathies. Variants in TUBB2A have been reported in 10 patients with a broad spectrum of brain imaging features, ranging from a normal cortex to polymicrogyria, while one patient has been reported with progressive atrophy of the cerebellar vermis.
Methods In order to further refine the phenotypical spectrum associated with TUBB2A, clinical and imaging features of 12 patients with pathogenic TUBB2A variants, recruited via the international network of the authors, were reviewed.
Results We report 12 patients with eight novel and one recurrent variants spread throughout the TUBB2A gene but encoding for amino acids clustering at the protein surface. Eleven patients (91.7%) developed seizures in early life. All patients suffered from intellectual disability, and 11 patients had severe motor developmental delay, with 4 patients (36.4 %) being non-ambulatory. The cerebral cortex was normal in five individuals and showed dysgyria of variable severity in seven patients. Associated brain malformations were less frequent in TUBB2A patients compared with other tubulinopathies. None of the patients had progressive cerebellar atrophy.
Conclusion The imaging phenotype associated with pathogenic variants in TUBB2A is highly variable, ranging from a normal cortex to extensive dysgyria with associated brain malformations. For recurrent variants, no clear genotype–phenotype correlations could be established, suggesting the role of additional modifiers.
- neurosciences
- clinical genetics
- epilepsy and seizures
- neurology
- genetics
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Human cerebral cortical development requires precise regulation of neuronal proliferation, migration and differentiation, as well as axon growth and guidance.1
Microtubules play a key role in these processes. Tubulin genes encoding for the different tubulin isotypes are highly expressed during cortical development.2 Alpha and beta tubulins form heterodimeric polymers that serve as a scaffold for the cytoskeleton dynamics required during cell division, migration and intracellular transport.3 The assembly of polymers requires GTP, and GTP hydrolysis is necessary for the dynamic properties of microtubules. Nevertheless, straightening of the tubules is likely to be the result of the assembly of the microtubule lattice and not of GTP metabolism.4 Microtubule function also depends on interaction with microtubule-associated proteins (MAPs).5 Functional heterogeneity is further increased by a number of post-translational modifications, for example, glutamylation and detyrosination.6
Variants in TUBA1A, TUBB2A, TUBB2B, TUBB, TUBB3 and TUBG1 have been linked to a spectrum of cortical malformations and associated brain malformations commonly referred to as tubulinopathies.7–9 Protein structures within the tubulin superfamily show a high degree of similarity. However, the phenotypical differences associated with variants in the various tubulin isotypes support the hypothesis that each tubulin has a distinctive function.3 10 Additionally, tubulin isotypes are not interchangeable as shown, for example, for TUBB3.11
TUBB2A is a neuronal-specific isotype of beta-tubulin, but the expression of TUBB2A during gestation has been reported to be lower compared with other beta tubulin isotypes. This finding suggests a minor role of TUBB2A in brain development.2 12 Nevertheless, to date, six patients with variants in TUBB2A have been reported with a heterogeneous spectrum of brain malformations, described as pachygyria, polymicrogyria, simplified gyral pattern (SGP) and dysgyria. The presence of associated brain malformations, as well as clinical features such as epilepsy and motor and intellectual disability, also varies in severity between the reported patients.13–16Three additional patients have been reported, but clinical information is limited to infantile spasms with normal brain imaging in one patient,17 while for the other two patients, abnormalities of the nervous system have not further been specified.18 Recently, a variant in TUBB2A has also been described in a patient with progressive atrophy of the superior cerebellar vermis and thinning of the corpus callosum with the clinical presentation of progressive spastic paraparesis and polyneuropathy, consistent with a neurodegenerative process.19
The underlying pathogenic effects of variants on protein function are poorly understood. Although effects on polymerisation, integration into the microtubule scaffold or assembly at the spindle pole during mitosis have been suggested, the heterogeneous phenotypes are likely caused by residue-specific effects on cortical development. Additionally, patients with recurrent variants but differing phenotypes indicate the presence of additional modifiers.16 19
The aim of this work was to further delineate the clinical and imaging features associated with pathogenic variants in TUBB2A in 12 novel patients, in combination with a review of the literature.
Methods
Patients were recruited through the international network of the authors, COST Action CA16118 Neuro-MIG.
Clinical data were collected by a review of the patient’s medical records and clinical examination. MRI images were reviewed by SB, TV and ACJ, when available. Particular attention was spent on the type, severity and the anterioposterior severity gradient, and anatomical distribution of abnormal cortical lamination and associated brain malformations. Dysgyria is defined as a cortical malformation consisting of variable sulcal depth and/or orientation without blurring of the grey-white matter interface and with normal cortical thickness.20 21
Peripheral blood samples were obtained from all patients for genetic testing. DNA was extracted using standard protocols, specific for each centre. Genetic testing was performed using capture-based methods, either through gene panel analyses (samples 1–4) or whole-exome sequencing (samples 5–12), after which the presence of the variant was confirmed by Sanger sequencing in all patients except for patient 7. The absence of the variants in the parents were also confirmed by trio analysis or Sanger sequencing for all patients.
Results
Clinical features
Clinical findings are summarised in table 1. All patients presented with global developmental delay. Motor development was severely affected in all but one patient (91.6%), and four of these patients (36.4%) were non-ambulatory at ages 5.0, 2.5, 11.0 and 15.0 years, respectively. Spastic paraplegia or cerebellar signs were not reported in this cohort. Eight patients were non-verbal, while four had very poor speech limited to a few single words. One patient was reported to have cortical blindness. Eleven patients (91.6%) had epilepsy, with age of onset varying from the neonatal period up to the age of 5 years. In seven patients, seizures were generalised, four of which presented with infantile spasms. Four patients were refractory to treatment. Five patients (5/10, 50%) had postnatal microcephaly (−2.5 SD and –4.5 SD) and five patients were normocephalic. Six patients (6/10, 60%) presented with mild dysmorphic facial features, while four patients were not dysmorphic. Dysmorphic facial features included a high forehead and deep-set eyes (patient 2) and a round face with a flat nasal bridge, cupid upper lip and full lower lip in patient 3. Dysmorphic features were not further specified for patients 1 and 4.
Imaging
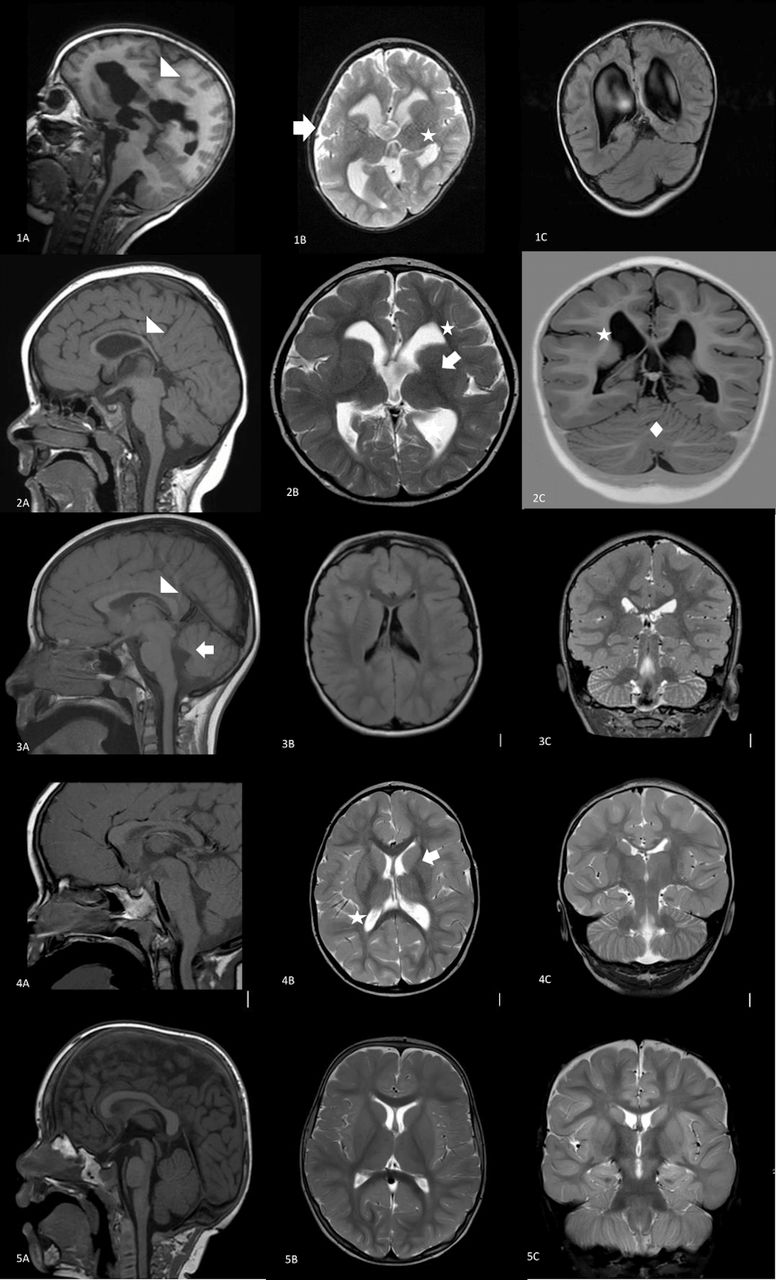
MRI of the brain was performed in all patients between ages 2 days and 12 years (table 1 and figures 1 and 2). MRI images were available for review for nine patients (P1–9). We included three additional patients (P10-12) in which clinical and imaging data were retrieved from the patient files but images were not available for review by the authors. Brain MRI was normal for one patient (P1) and revealed a spectrum of brain malformations in the others. The cerebral cortex was reported to be normal in five patients (41.7%), although focal cortical heterotopia was mentioned in one. Seven patients (58.3%) had tubulinopathy-related dysgyria, closely resembling polymicrogyria in two patients (P6 and P7). The parietal and temporal regions were most severely affected in most patients. No recurrent pattern of the anatomical distribution of the malformations could be observed. The lateral ventricles were enlarged in eight patients (66.7%), and in patients 6 and 7, the lateral ventricles had a hooked appearance. The brainstem was normal in all patients. The corpus callosum was abnormal in eight patients (66.7%) and the basal ganglia were dysmorphic in four patients (33.3%). Four patients (33.3%) had mild hypoplasia of the cerebellar vermis and/or a dysmorphic vermis; the cerebellar hemispheres were hypoplastic in one patient.

Brain imaging findings with midline, axial and coronal sections of patients with TUBB2A variants and a normal subject. Patient 1 at age 5 years does not present any brain malformations (1A–C). Patient 2 showing mild dysgyria (arrow denotes fronto-orbital, and asterisk denotes parahippocampal) and a dysmorphic CC (arrowhead) (2A–C). Patient 3 at age 2 months presenting with severe dysgyria (arrows), dysmorphic CC (arrowhead) and BG (asterisk) (3A–C). Patient 4 at age 1 year 11 months (sagittal) and 7 years (axial and coronal) presenting with mild dysgyria (arrows) and a mildly dysmorphic CC (arrowhead) (4A–C). Patient 5 at age 10 months had a normal cortex and hypoplasia of the CC (arrowhead). The white matter was reduced (arrows) (5A–C). BG, basal ganglia; CC, corpus callosum.
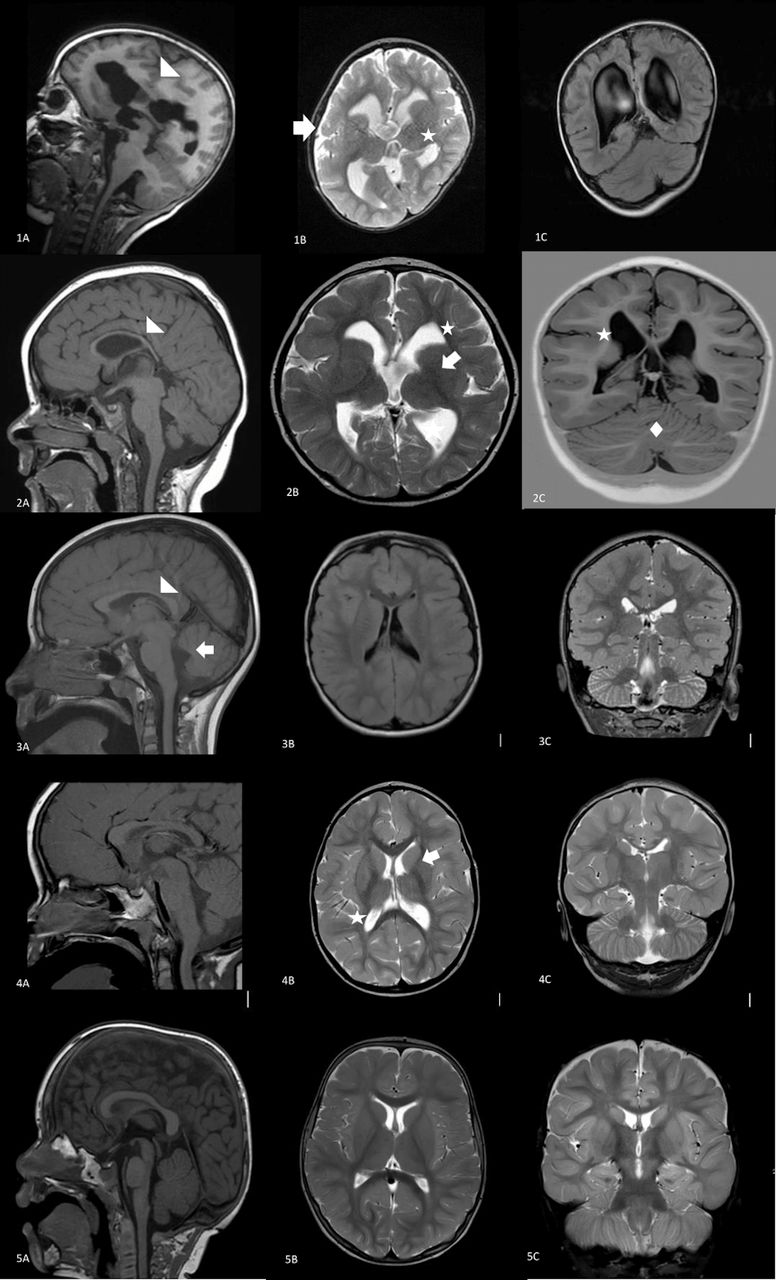
Patient 6 presented with severe bilateral dysgyria (arrow), partial agenesis of the CC (arrowhead) and dysmorphic BG (asterisk) (1A-C). Patient 7 at age 10 months had generalised dysgyria, dysmorphic BG (asterisk), hypoplastic CC (arrowhead), dysgenesis of the cerebellar vermis (diamond), hooked lateral ventricles and reduced white matter volume (arrows) (2A–C). Patient 8 at 8 years 1 month has a normal cortex, mildly enlarged lateral ventricles, hypoplasia of the CC (arrowhead) and vermis hypoplasia (arrow) (3A–C). Patient 9 at age 3 years 7 months presenting with a normal cortex,mildly enlarged posterior horns of the lateral ventricles, mildly dysmorphic basal ganglia (asterisk) and reduced white matter (arrow) (4A–C). Healthy control at age 13 months (5A–C). BG, basal ganglia; CC, corpus callosum; M, months; Y, years.
Clinical and imaging features of patients with variants in TUBB2A
Genetics
Whole-exome sequencing or gene panel analysis was performed in 12 unrelated patients with neurodevelopmental delay with or without brain malformations. The parents were either tested in parallel with the patients (trios) or in a second step by Sanger sequencing. We detected nine pathogenic or likely pathogenic variants in TUBB2A (Genomic RefSeq accession: NC_000006.11; mRNA RefSeq accession: NM_001069.2), one of which has previously been reported in the literature. All variants in TUBB2A occurred de novo in the index patients. No additional pathogenic or likely pathogenic variants were detected.
The previously reported p.(Ala248Val) variant detected in patients 8, 9 and 12 has been reported multiple times.13 15 18 Patients 1 and 3 carried novel missense variants p.(Val49Gly) and p.(Val49Met), respectively, that affect the same amino acid but result in different substitutions. Patients 6 and 7 carry the same not previously reported p.(Pro357Leu) variant.
The variants were spread over the TUBB2A gene affecting amino acids throughout the TUBB2A protein (figure 3) and were all located at highly conserved amino acid positions.22 Although TUBB2A is largely made up of sheets and helixes, the majority of variants are located in the random coils between those secondary structures (figure 3). Only the p.(His396Tyr) variant in patient 2, the p.(Glu410Lys) in patient 10 and the p.(Asp417Asn) reported by Sferra et al 19 are located in the two last helices of the protein, which are part of the c-terminal MAP-binding domain. Nevertheless, all variants were predicted to have a deleterious effect on protein function. When looking at the 3D protein structure, variants appear to cluster at the protein surface, suggesting an impact on protein 3D structure and lateral interactions (figure 3).

{kind=link}
{kind=link}
{kind=link}
Distribution of variants in the TUBB2A protein structure. Functional domains are highlighted in the 3D model (A) and the linear model (B): green,helices; blue, sheets. Reported variants from this cohort and variants reported in the literature are written in black in the 3D model and blocked in red in the linear model. Variants reported in ClinVar without further clinical information are written in red in the 3D model and are blocked in yellow in the linearmodel. The 3D structure is based on Swiss model TBB2A_HUMAN Q13885 tubulin beta-2A chain.
Discussion
Tubulinopathies have been associated with a spectrum of cortical malformations with associated brain malformations often including dysmorphic basal ganglia, thin corpus callosum and brainstem and/or cerebellar vermis hypoplasia.7 20 Variants in TUBB2A have previously been reported in patients with variable clinical and cortical imaging features, ranging from a normal cortex to polymicrogyria.13–18 Additionally, one patient has been reported with progressive neurodegeneration and loss of independent walking but without cortical malformations.19 Furthermore, neurodegeneration has been reported for variants in TUBB3 causing adult-onset polyneuropathy and for TUBA4A causing familial amyotrophic lateral sclerosis.23 24 As five patients in our cohort have a normal cortex but are significantly younger (2–12 years at last examination) than the patient reported by Sferra et al,19 further follow-up is needed to assess for features of early-onset neurodegeneration. There was a strong overlap between the severity of motor developmental delay and imaging findings as patients with severe cortical malformations in our cohort were non-ambulatory, whereas patients with mild or without cortical malformations had severe motor delay but were able to walk with support. Further study and long-term follow-up are needed to assess whether the phenotype can be divided into two groups: (1) severely affected, non-ambulatory patients with severe forms of malformations of cortical development (MCD)and (2) initially ambulating patients, possibly with neurodegeneration causing progressive spastic paraplegia, and with mild or without MCD.
Our findings suggest that absent speech is a common feature of TUBB2A. Epilepsy was present in all but one patient in our cohort (P10) and in six patients reported in the literature for which this information was available (17/20 patients, 85%). Interestingly, epilepsy was clinically suspected in patient 10 in our cohort, presenting with mild dysgyria, but could not be confirmed by long-term EEG. Although the reported series remains small, the incidence of epilepsy seems higher in patients with TUBB2A compared with other tubulinopathies.7 25 Microcephaly and visual impairment are variably present. Mild dysmorphic features were present in six (60%) of our patients where this information was available and in one previously reported patient, which is in line with findings in other tubulinopathies.16 26 27
Our cohort includes 12 additional patients with 8 previously unreported variants in TUBB2A. Brain imaging confirms the heterogeneous spectrum that occurs in patients with variants in TUBB2A ranging from a normal cortex to severe dysgyria. This finding should lead to considering TUBB2A variants not only in patients with typical imaging findings suggestive of a tubulinopathy but also in patients with developmental delay, epilepsy and mild brain malformations, with or without involvement of the cortex. Especially subtle features of brain malformations can easily be missed on MRI. Therefore, we would like to stress the importance of reviewing imaging data when a variant in TUBB2A is detected during molecular investigations, a process called reverse phenotyping. Imaging and clinical findings have been reported to show mild asymmetry of white matter reduction and pyramidal findings, respectively.13 15 However, asymmetry has not been observed in our cohort and is uncommon in other tubulinopathies. The brainstem is normal in all patients included in our cohort, and cerebellar hypoplasia or vermis dysplasia occurred in only four patients (33.3%). This contrasts with the high incidence of cerebellar hypoplasia reported for other tubulinopathies.20 Dysmorphic basal ganglia, considered a key feature of tubulinopathies, was present in only four patients in our cohort and in one patient reported in the literature, thus contrasting the high incidence reported in other tubulinopathies.7 13
Several recurrent variants in the TUBB2A gene have been observed, suggesting mutational hotspots. For the recurrent p.(Ala248Val) observed in our cohort and the literature, no clear genotype–phenotype correlations could be established. The imaging phenotype associated with the variant at p.(Ala248Val) is heterogenous and varies from mild brain malformations as seen in patients 8 and 9 and reported by Cushion et al,13 to severe malformations as in patient 12 and as reported by Rodan et al.15 For the patient reported by Retterer et al,18 no information of brain imaging is available. Furthermore, variants affecting positions 246 and 247 have been described in patients with infantile spasms and SGP, respectively.13 17 Clinical and imaging features were heterogenous in patients 1 and 3, both carrying variants affecting the same location within the protein, c.145G>A, p.(Val49Met) and c.146T>G, p.(Val49Gly), respectively. Patient 1 appears to have no brain malformations; patient 3 was severely affected, with MRI revealing severe dysgyria, partial corpus callosum agenesis and dysmorphic basal ganglia. Overlapping clinical and imaging features are present in the severely affected patients 6 and 7 in our cohort, both carrying the p.(Pro357Leu) variant. Both patients have bilateral diffuse dysgyria, abnormal corpus callosum, basal ganglia and cerebellum. The variability of genotype and phenotype is likely linked to additional modifiers such as environmental factors or variable gene expression.
Expression of TUBB2A in the developing brain has been reported to be less than that of other beta-tubulin isotypes, suggesting a minor role of TUBB2A in brain development.12 More specifically, the role of TUBB2A in neuronal migration has been suggested to be less pronounced compared with TUBA1A and TUBB2B.8 As variants in the different isotypes lead to unique as well as overlapping phenotypes, variants are likely to selectively affect particular subsets of neurons.
Variants in TUBB2A are distributed through the entire gene. Six of all reported variants are located in the GTPase domain, whereas seven are located in the two-layer sandwich domain. Interestingly, when considering the 3D model, variants seem to cluster close to one surface site of the protein, leading to the hypothesis that the 3D protein structure is altered, causing a change in the dynamic capabilities and lateral interactions by changes in the surface structure. Variants in the carboxy-terminal domain have been shown to alter microtubule function28 and have been reported in TUBA1A,27 TUBB3 23 and TUBG1.10 The p.(Asp417Asn) variant interferes with the interaction of TUBB2A with KIF1A impairing the assembly of spindle poles during mitosis, which ultimately leads to accumulation of mitotic cells with aberrant spindle figures. However, this has also been observed for the p.(Ala248Val) variant, although to a lesser extent.19
In conclusion, this patient cohort expands the phenotypical spectrum associated with variants in TUBB2A to both milder and more severe ends, highlighting the heterogeneity of clinical and imaging features. As for counselling, variants in TUBB2A therefore need to be considered in patients with severe clinical and brain imaging abnormalities, as well as in patients with neurodevelopmental delay and/or epilepsy and MRI reported as normal.
References
Footnotes
Contributors ACJ and KK conceived the work. SB, TV, KS and ACJ assisted with data acquisition. SB, ACJ and KS drafted the manuscript, which was revised and approved by all.
Funding Recruitment and sequencing of patient 11 was supported by the The Australian Genomics Health Alliance, which is funded by National Health and Medical Research Council and the Australian Government’s Medical Research Future Fund. ACJ is supported by a Senior Clinical Investigator Fellowship from FWO. SB, RR, GMSM, RL, GMM, WBD, NBB, MM, ACJ and KS are members of Neuro-MIG, the European Network for Brain Malformations, supported by COST (Action CA16118, www.neuro-mig.org). Published with the assistance of the Fondation Universitaire de Belgique.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval The study was approved by the ethical committee of the UZ Brussel (BUN 143201214360). Prior to genetic testing, informed consent was obtained from all families.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included in the article or uploaded as supplementary information. Data are available on reasonable request. Main data relevant to the study are included in the article.