Article Text

Abstract
Background Data on the long-term motor outcomes of genome-wide association study (GWAS)-linked Parkinson disease (PD) carriers are useful for clinical management.
Objectives To characterise the association between GWAS-linked PARK16 gene variant and disease progression in PD over a 9-year time frame.
Methods Over a 9-year period, carriers of PARK16 rs11240572 variant and non-carriers were followed up and evaluated using the modified Hoehn and Yahr (H&Y) staging scale and Unified Parkinson’s Disease Rating Scale (UPDRS) part III. A longitudinal, linear mixed model was performed to compare the changes of H&Y staging scale, UPDRS motor score and UPDRS subscores between the two groups.
Results A total of 156 patients (41 PARK16 carriers and 115 non-carriers) were evaluated and followed up for up to 9 years. Using longitudinal linear mixed model analysis, there was a greater rate of deterioration in the motor function as measured by the UPDRS scores compared with non-carriers after 5 years from the date of diagnosis (p=0.009). In addition, we demonstrated that PARK16 variant carriers had worse gait scores (p=0.043) and greater motor progression than non-carriers after 6 years based on the modified H&Y staging scale (p=0.040).
Conclusions In a 9-year longitudinal study, we demonstrated that PD PARK16 variant carriers exhibited greater motor progression after 5 years of disease compared with non-carriers, suggesting that GWAS-linked gene variants may influence disease progression over time. Closer monitoring and management of these higher risk patients can facilitate a better quality of life.
- parkinson disease
- motor progression
- GWAS
- Park 16
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Parkinson disease (PD) is a progressive neurodegenerative disorder underpinned by both genetic and environmental factors. Genetic studies using a variety of methods including linkage analysis and exome sequencing have shed light on the pathophysiology of monogenic PD.1 A study suggested that genetic factors could account for up to 27% of the PD causes rather than estimated 3%–5% attributed to single-nucleotide polymorphisms identified in genome-wide association studies (GWAS).2 Hence, genetic factors may assume a greater role in modulating PD risk and disease progression.
A GWAS study in Japan identified Park16 locus to be associated with PD.3 This finding has been replicated by multiple groups from Europe, Malaysia, Chile and also in the Jewish population.4 Within PARK16 locus, we previously demonstrated that the PARK16 rs11240572 variant was most robustly associated with the modulating risk of PD in our Chinese population.5 The robust association with this variant was subsequently replicated in other independent Han Chinese PD cohorts,4 including a pooled analysis.6
As GWAS-linked variants are intronic (they do not code for a protein), their pathophysiological significance and clinical relevance are usually unclear. Furthermore, genetic association studies are generally cross-sectional in nature and the clinical impact of GWAS intronic variants on disease progression has not been properly addressed. Most functional and clinical studies in patients with PD focus on carriers with common or recurrent coding mutations/variants. To address these gaps in knowledge, we conducted a 9-year prospective longitudinal study to elucidate the clinical impact of the Park16 rs11240572 variant (which has been consistently replicated as a disease-associated variant in the Chinese population) to determine if the clinical progression of the carriers differs from non-carriers in our Chinese population.
Methods
Patients and setting
Patients with PD were assessed prospectively from movement disorder outpatient clinics at the National Neuroscience Institute over a 9-year period. The SingHealth Centralized Institutional Review Board approved the study. All subjects gave written informed consent.
Genetic analyses
We genotyped the PARK16 rs11240572 variant using the Illumina Human OmniZhonghua-8 v1A BeadChip. All positive variants in our selected samples have been validated by Sanger sequencing. Patients with PD were categorised according to the genotyping results into carriers (PARK16 rs11240572 A allele, including AC and AA.) and non-carriers (PARK16 rs11240572 homozygous C allele).
Data collection and assessments
We collected demographic data from all subjects. Total daily levodopa equivalent doses were calculated from PD medications used by patients at years 2 and 5. Modified Hoehn and Yahr (H&Y) staging scale and Unified Parkinson’s Disease Rating Scale (UPDRS) part III were used to assess disease severity and motor conditions, respectively. UPDRS motor subscores of the cardinal features of tremor (items 20 and 21), rigidity (item 22), bradykinesia (items 23–26 and 31), and postural and gait abnormality (items 27–30) were calculated, respectively. UPDRS scores were obtained during the ‘on’ medication period. The assessments were evaluated by the specialist on the same day at baseline and follow-up visits. The follow-up visits were carried out yearly and the final visit was up to 9 years. Both clinicians and patients were blinded to genotype status.
Statistical analysis
The differences from baseline versus years after diagnosis in PARK16 rs11240572 variant carriers were compared with non-carriers by means of a longitudinal, linear mixed model. Statistical significance was set at p<0.05. Statistical analysis was performed using SAS V.9.3.
Results
A total of 156 patients (115 non-carriers who carried CC allele and 41 PARK16 rs11240572 variant carriers, including 2 patients carried AA and 39 patients harboured AC) were evaluated and followed up for up to 9 years. Patients from both groups were not significantly different in terms of demographic information and other clinical assessments at baseline (all p>0.05) (table 1).
Comparison of demographic and baseline clinical data between two groups
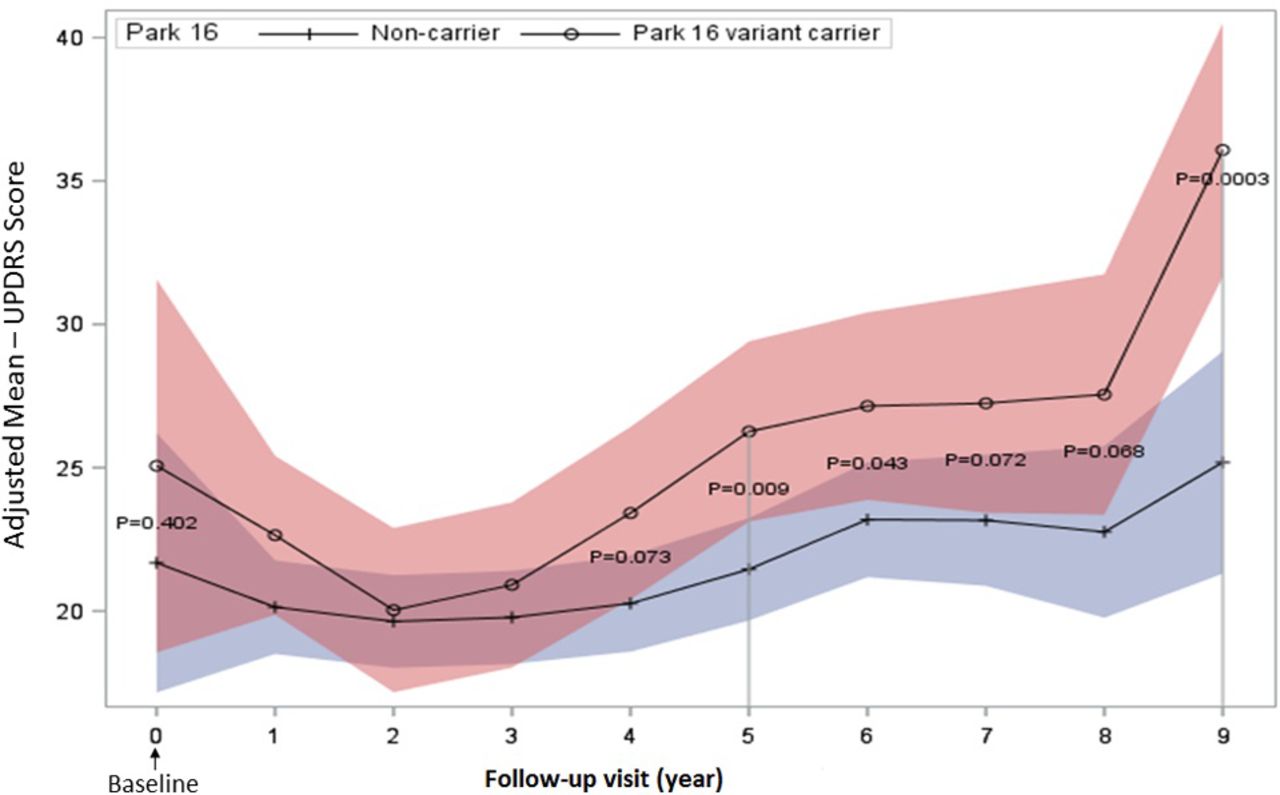
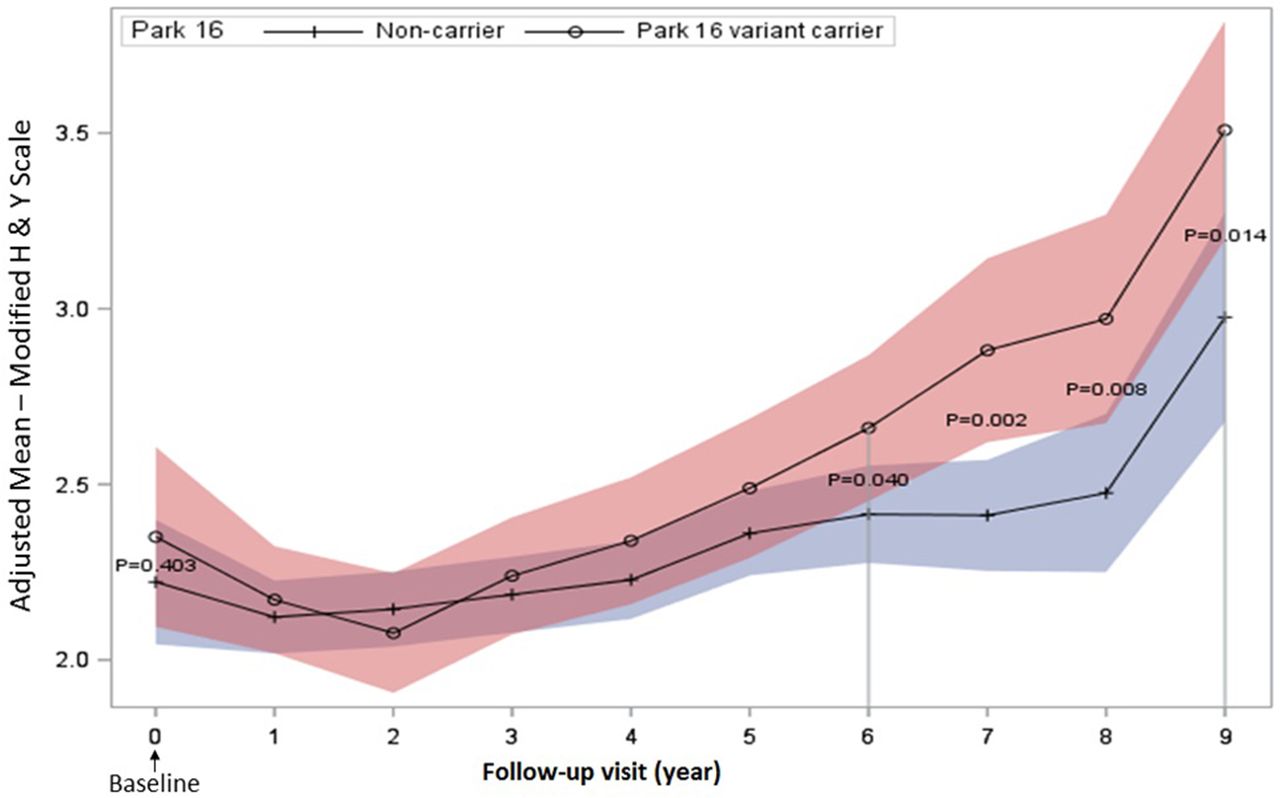
The mean UPDRS motor scores were consistently higher in carriers compared with non-carriers at yearly evaluation for 9 consecutive years (figure 1). Using the longitudinal linear mixed model analysis, we demonstrated that PARK16 rs11240572 variant carriers had higher UPDRS motor scores than non-carriers at 5 years after diagnosis (p=0.009). The p values of the difference between two groups in years 7 and 8 were borderline and the difference became significant again in year 9 (p=0.0003). The carriers experienced worse UPDRS gait score than non-carriers at year 6 of PD (p=0.043) and the difference became more substantial from then onwards (figure 2). The carriers also experienced faster progression than non-carriers at year 6 from diagnosis by using a modified H&Y staging scale (p=0.040) and the difference was consistently significant after 6 years (figure 3).

Progression of mean UPDRS motor score in carriers a non carriers. Comparisons of longitudinal model-based LS means reveals UPDRS motor scores in PARK16 carriers are higher than non-carriers from year 5 onwards. Shaded regions indicate 95% CIs on LS (adjusted) means. LS, least squares; UPDRS, Unified Parkinson’s Disease Rating Scale.

Progression of mean posture and gait score in carriers and non-carriers. Comparisons of longitudinal model-based LS means showing PARK16 carriers have higher posture and gait scores than non-carriers from year 6 onwards. Shaded regions indicate 95% CIs on LS (adjusted) means. LS, least squares; PIGD score, posture and gait score.

{kind=link}
{kind=link}
{kind=link}
Progression of modified H&Y scale in carriers & non-carriers. Comparisons of longitudinal model-based LS means demonstrating PARK16 carriers experience worse H&Y scale than non-carriers from year 6 onwards. Shaded regions indicate 95% CIs on LS (adjusted) means. H&Y scale, Hoehn and Yahr scale; LS, least squares.
Discussion
This current long-term (over 9 years) longitudinal study evaluated the association between a PD GWAS-linked intronic variant and clinical progression using a standardised methodology where clinical assessors were blinded to the genotype information. We formulated our hypothesis based on our earlier observation of a robust association between PARK16 rs11240572 variant and PD, a finding that was confirmed in other independent Chinese cohorts.5 6 In the current study, we showed that the UPRDS motor scores in PARK16 rs11240572 variant carriers were consistently higher than in non-carriers over the 9-year period. Statistically significant worse UPDRS motor scores in carriers compared with non-carriers were seen after 5 years from the date of diagnosis. The deterioration was also evident on the modified H&Y staging scale and UPDRS gait score after 6 years, indicating that the association between PARK16 rs11240572 variant and patients with prominent gait disorder symptoms. Our previous study reported that a significantly higher proportion of patients with PD with postural instability and gait disorder had a positive PD family history.7 It may be useful to further screen PARK16 rs11240572 variant among patients with PD who are likely to be postural instability and gait disorder (PIGD) subtype.
The mechanism by which PARK16 rs11240572 variant contributes to the faster motor progression of PD is unclear. However, it is possible that PARK16 rs11240572 variant is in linkage disequilibrium with another causative gene within the PARK 16 locus. Clues may be obtained by looking at the functions of adjacent genes around PARK16 rs11240572 variant. Identification of a candidate gene for the PARK16 locus may be achieved through targeted resequencing of PARK16 locus. Thus, further detailed sequencing and functional genomic studies will be required to pinpoint the causative gene and elucidate its underlying mechanism.
Clinico-genetic correlations to determine factors modulating clinical progression have been carried out with monogenic forms of PD. As an illustration, a recent longitudinal study in Asian patients with PD demonstrates a faster decline in motor UPDRS scores among those with LRRK2 risk variant-associated PD.8 This study and our current report suggest that genetic factors may have a modulatory effect on disease onset and progression, although it is unclear how the genetic profile of an individual, consisting of numerous genetic variants, influence PD development. Furthermore, there are several potential confounding variables (such as lifestyle and environmental factors) that need to be further investigated.
In conclusion, we have shown in a long-term longitudinal study over 9 years that PARK16 rs11240572 variant (a GWAS-linked variant) carriers with PD were associated with a greater motor progression compared with non-carriers. Our study provides useful clues for future efforts to explore the possible mechanism underlying Park16-related PD, and suggests potential benefits for closer monitoring and better management of these carriers as the disease progresses. We also provide proof of principle that long-term evaluation of GWAS-linked intronic variant carriers can have potential clinical relevance. We acknowledge that sample size may be a potential limitation in our study. Validation of our findings in larger cohorts and determination of collective effects of genetic factors on PD progression will be warranted.
Acknowledgments
The authors thank the National Medical Research Council (STaR Award and Translational Clinical Research Programme in PD). The authors thank Samuel Ng Yong Ern for data management.
Footnotes
XD and BX contributed equally.
Contributors XD and BX: analysis and interpretation of data, statistical analysis, drafting/revising the manuscript. JCA: statistical analysis, drafting/revising the manuscript. EN and JNF: acquisition of data. Y-LL: acquisition of data, interpretation of data, drafting/revising the manuscript. E-KT and LCST: study concept and design, acquisition of data, drafting/revising the manuscript, study supervision and coordination, obtaining funding.
Funding This research is supported by the Singapore National Research Foundation under its Translational and Clinical Research Flagship Programme.
Competing interests No competing interests.
Provenance and peer review Not commissioned; externally peer reviewed.
Patient consent for publication Obtained.